What is Haemorrhoidectomy?
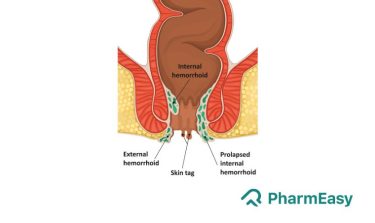
Haemorrhoidectomy is the surgical removal of haemorrhoids, commonly called piles. Haemorrhoids are a condition characterised by swollen veins in the anal and rectal region. Depending upon the location of haemorrhoids, these can be internal (inside the rectum) or external (around the anal opening. Haemorrhoids are managed using both non-surgical and surgical treatment along with lifestyle modifications. Usually, haemorrhoids which are recurrent, prolapsed (falling outside the rectum) and the ones which require reduction (shrinkage of haemorrhoidal mass) are often surgically removed by haemorrhoidectomy.1
Diagnosis
Medical History and Physical Examination
Your doctor will take a detailed history and do a thorough physical examination before diagnosing haemorrhoids. He may do a digital rectal examination and a few imaging tests. Depending upon the type of haemorrhoid and the severity, he/she will decide the need for surgical excision of the haemorrhoid.1,2
Indications for Haemorrhoidectomy
Following are the indications for haemorrhoidectomy:1
- If there is no improvement after non-operative management (medications and lifestyle modifications)
- Haemorrhoids that show bleeding
- Severe haemorrhoids like recurrent haemorrhoid, clot in a haemorrhoid unresponsive to medications
- Mixed haemorrhoids (both internal and external haemorrhoid) that bulge out
- Incarcerated haemorrhoids (prolapsed internal haemorrhoids)
- Thrombosed haemorrhoids in which a blood clot is formed inside the haemorrhoid.2
Treatment
In this section, we will look at the different types, procedures, available for haemorrhoidectomy:
Types of haemorrhoidectomy:
- Open haemorrhoidectomy or Milligan-Morgan haemorrhoidectomy wherein the haemorrhoid is surgically removed and the wound is left open to heal.1
- Closed haemorrhoidectomy also called as Ferguson haemorrhoidectomy in which the wound is closed with a suture.1
- Stapler haemorrhoidectomy (SH) also known as procedure for prolapsed haemorrhoids (PPH) which involves excision of the haemorrhoidal tissue and use of a stapling procedure to lift the haemorrhoid back to the normal position.3
- LigaSure haemorrhoidectomy 3
- Cryosurgical haemorrhoidectomy which uses nitrous oxide to freeze and remove haemorrhoidal tissue.4
- Laser haemorrhoidectomy uses laser to shrink the haemorrhoids.4
- Harmonic ultrasonic scalpel haemorrhoidectomy4
- Clamp and cautery haemorrhoidectomy4
- Submucosal haemorrhoidectomy4
- Whitehead’s circumferential haemorrhoidectomy4
- Bipolar diathermy haemorrhoidectomy4
- Starion haemorrhoidectomy4
Before performing haemorrhoidectomy, you will be given an enema for bowel clearance. It should not be painful but will make you little uneasy and uncomfortable. Haemorrhoidectomy procedures are carried out after anaesthetizing the patient with local anesthesia. The surgery procedure is usually carried out in prone jack-knife position, which requires you to lie on your stomach on a table which is flexed at 90 degrees. Your head and body will be lowered and your hips will be raised.1
The duration of hospital stay for stapled haemorrhoidectomy is one day; whereas conventional haemorrhoidectomy may require hospitalization for 6-7 days and the duration of laser surgery is short and requires no hospitalisation. As haemorrhoidectomy may require immobilization temporarily, you should always go to the hospital along with a family member or caretaker.5
Post-operative medications:
- Stool softeners may help reduce straining associated with constipation.
- Topical treatment with ointments may help reduce pain and swelling.
- Your doctor may prescribe suppositories, pills, creams and wipes for symptomatic relief.
- Your doctor may prescribe you antibiotics post-surgery that should be taken sincerely.3,4
Points to be kept in mind after haemorrhoidectomy: 6
- Dietary and lifestyle modifications: increased intake of oral fluids (5-6 glasses of water or any other non-caffeinated beverage) and dietary fibers like fruits, vegetables, lentils, etc, mild-moderate intensity exercises and refraining from straining activities like weight lifting.
- A good anal hygiene should be practised that includes washing after defecation and avoid using soaps to wash the anal area as this can result in dry and itchy skin.
- You should avoid self-medicating as they can cause hard stools and constipation which may lead to tearing of tissues in the anus.
- For the next few weeks, you may experience mild bleeding in stool. You can place new gauze over the wound if the older one becomes soiled. In case of heavy bleeding, you should contact your physician.
- Your physician may advise you to apply antibiotic ointments to the site daily for the first week after surgery. In case of surgical-site redness, swelling or foul-smelling drainage, contact your doctor.
- A twenty-minute sitz bath which involves soaking the affected area in a tub of warm water to aid healing.
- After surgery, ensure your bowel remains soft. This can be done by increasing the intake of oral fluids and taking a high-fibre diet.
Risks
- Open haemorrhoidectomy may increase the risk of urinary retention, pain, thrombosed haemorrhoids and bleeding.1
- Late onset complications may include the risk of recurrent haemorrhoids, skin tags, narrowing of the anal canal (anal stenosis).1
- Although rare but haemorrhoidectomy may also increase the risk of abscess formation, sepsis, excessive bleeding and inflammation of the abdominal wall.1
- Stapler haemorrhoidectomy may increase the risk of fluid leakage from the surgical site, Fournier’s gangrene (bacterial infection of penis, scrotum) and pelvic sepsis.3
- Cryosurgical haemorrhoidectomy may increase the risk of discharge and edema.4
Haemorrhoidectomy is contraindicated in the following conditions: 1
- Uncontrolled bleeding disorder
- Portal hypertension (high pressure in a vein which supplies blood to the liver)
- Inflammatory bowel disease
- Faecal incontinence (not able to control bowel movements)
- Any medical condition which makes the patient unable to undergo anesthesia
- Rupture of the wall between rectum and vagina in women
Also Read: Is Anal Sex Safe? A Comprehensive Guide to Risks and Safety Measures
Conclusion
Haemorrhoids or piles can be managed using different treatment modalities. The surgical excision of haemorrhoids is called as haemorrhoidectomy. Different types include conventional haemorrhoidectomy (open and close), laser, LigaSure, cryosurgical, stapled haemorrhoidectomy, etc. Each type has its own benefits and risks. Your doctor or proctologist will assess the need of the surgery and weigh the benefits against the risks involved.
Frequently Asked Questions:
What is haemorrhoidectomy?Haemorrhoidectomy is the surgical removal of haemorrhoids.
Does haemorrhoidectomy pain?Yes, haemorrhoidectomy is associated with post-operative pain; but you need to worry your doctor will prescribe painkillers for managing pain.3
What are the types of haemorrhoidectomy?The different types of haemorrhoidectomy including open, closed , laser , LigaSure , stapled , cryosurgical , harmonic ultrasonic scalpel, clamp and cautery , submucosal, whitehead’s circumferential, bipolar diathermy LigaSure and Starion haemorrhoidectomy types.4
What are the contraindications of haemorrhoidectomy?Haemorrhoidectomy is contraindicated in uncontrolled bleeding disorders, portal hypertension, Ulcerative colitis or Crohn’s disease, faecal incontinence (not able to control bowel movements) or any medical condition which makes the patient unable to undergo anesthesia.1
What is the risk after haemorrhoidectomy?Haemorrhoidectomy may increase the risk of urinary retention, pain, thrombosed haemorrhoid and bleeding.1
Disclaimer
The information provided at this site is for educational purposes only and is not intended to be a substitute for medical treatment by any healthcare professional. As per unique individual needs, the reader should consult his/her physician to determine the appropriateness of the information provided for his/her situation.
References:
- Cristea C, Lewis CR. Haemorrhoidectomy. InStatPearls [Internet] 2022 Jul 4. StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK549864/
- Holzheimer RG. Haemorrhoidectomy: indications and risks. European journal of medical research. 2004 Jan 26; 9(1):18-36. Available at: https://pubmed.ncbi.nlm.nih.gov/14766336/
- Yeo D, Tan KY. Haemorrhoidectomy-making sense of the surgical options. World Journal of Gastroenterology: WJG. 2014 Dec 12; 20(45):16976. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4258566/
- Agbo SP. Surgical management of haemorrhoids. Journal of surgical technique and case report. 2011 Jul; 3(2):68. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3296437/
- George R, Vivek S, Suprej K. How long to stay in hospital: Stapled versus open haemorrhoidectomy? Saudi Surgical Journal. 2016 Sep 1; 4(3):108. Available at: https://www.saudisurgj.org/text.asp?2016/4/3/108/193985
- Lohsiriwat V. Treatment of haemorrhoids: A coloproctologist’s view. World Journal of Gastroenterology: WJG. 2015 Aug 8; 21(31):9245. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4541377/




 Medically reviewed by Dr. Mayuri Pandey
Medically reviewed by Dr. Mayuri Pandey 
































Comments