
Introduction
Pregnancy is a critical time when the growing baby relies on the placenta to receive oxygen and essential nutrients from the mother’s bloodstream. In some cases, the placenta may attach itself to the bottom of the uterus, blocking the cervix, completely or partially, causing a condition called placenta previa. This condition makes it extremely difficult for the baby to be delivered vaginally, and it requires medical attention. The primary goal of treatment is to manage the symptoms and prolong the pregnancy until at least 36 weeks.
Let us explore more about placenta previa, its causes, symptoms, diagnosis, and treatment options in detail1.
Did you know?
- Internationally, Asian women have the highest prevalence of placenta previa with a total prevalence of 12.2 per 1000 pregnancies. The higher prevalence of placenta previa among Asian women compared to other populations could be due to genetic predisposition, environmental factors, and differences in lifestyle7.
- Pre-term delivery is considered optimum for women with placenta previa, with most cases delivering at about 36 weeks5,6.
Advertisement
Signs and Symptoms of Placenta Previa
The signs and symptoms of placenta previa can include:
- Bright red vaginal bleeding after 20 weeks of pregnancy, often without pain.
- Spotting followed by heavier bleeding.
- Painful pre-labor contractions of the uterus.
- Bleeding triggered by sexual intercourse or a medical examination.
- Bleeding that may not occur until labour with no clear trigger event2.
Placenta previa is a condition during pregnancy where the placenta blocks all or part of your baby’s exit from your vagina. The most common symptom is vaginal bleeding in the second half of pregnancy. People with placenta previa typically need a C-section delivery3.
Dr. M.G. Kartheeka, MBBS MD(Pediatrics)
Causes of Placenta Previa
The exact reason why placenta previa occurs is not known. However, research has shown that having scar tissue or damage in the lining of the uterus may increase the risk of developing this condition. This damage can be caused by a C-section or a surgery of the uterus done previously such as myomectomy (a surgery to remove non-cancerous growths called fibroids from the uterus, while leaving the uterus intact). It’s important to remember that not all women who have had these surgeries will develop placenta previa, and some women without any of these risk factors can still develop this condition3.
Risk Factors for Placenta Previa
There are several risk factors that can increase the likelihood of developing the condition:
- Previous cesarean delivery: Women who have had a previous cesarean delivery are at higher risk for placenta previa due to scarring in the uterus.
- Multiple pregnancies: Women carrying twins, triplets, or more are at higher risk of placenta previa due to the increased size of the uterus.
- Advanced maternal age: Women who are over the age of 35 are at higher risk of developing placenta previa.
- Smoking: Smoking during pregnancy can increase the risk of placenta previa.
- Previous uterine surgery: Women who have had previous uterine surgery, such as a myomectomy (surgery to remove uterine fibroids), are at higher risk of developing placenta previa.
- In vitro fertilization (IVF): Women who become pregnant through IVF are at higher risk of placenta previa due to the increased likelihood of multiple pregnancies and uterine abnormalities2,4.
Diagnosis of Placenta Previa
Placenta previa is typically diagnosed by pregnancy care providers using ultrasound imaging to check the position of the placenta in relation to the cervix. The following tests may be used to diagnose placenta previa:
- Vaginal ultrasound (transvaginal ultrasound): This involves inserting a transducer wand into the vagina to visualize the position of the baby, placenta, and cervix. This is the most accurate method for diagnosing placenta previa and is considered safe when performed correctly, even in the presence of bleeding.
- Abdominal ultrasound: This involves placing gel on the abdomen and using a handheld transducer to scan the outside of the belly.
Both types of ultrasounds produce images on a monitor or screen, allowing healthcare providers to determine the extent to which the placenta covers the cervix.
Advertisement
Placenta previa can be identified during a routine ultrasound at around 20 weeks of pregnancy, or it may be discovered if a person experiences symptoms such as vaginal bleeding.
If placenta previa is diagnosed, healthcare providers will monitor the placement of the placenta through regular ultrasounds and determine the appropriate treatment plan based on the extent of the condition2.
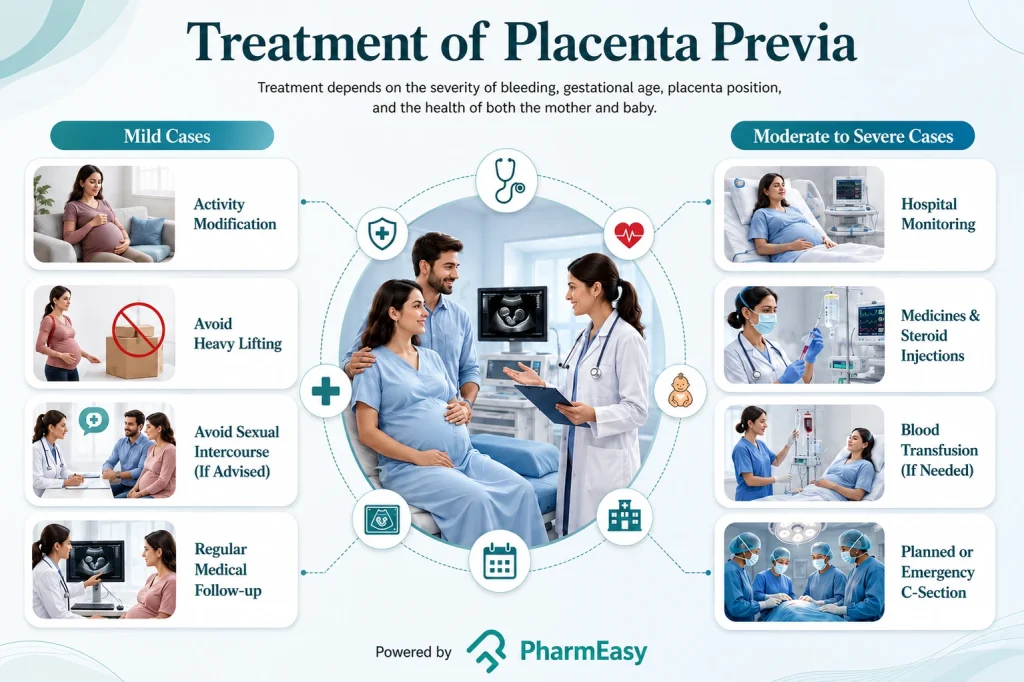
Treatment of Placenta Previa
Placenta previa treatment depends on several factors, including bleeding severity, gestational age, placenta position, and maternal and fetal health. Treatment options include:
Mild Cases
- Activity modification at home, such as avoiding heavy lifting, strenuous exercise, and sexual intercourse, as advised by your healthcare provider.
- Routine strict bed rest is generally not recommended, as it has not been shown to improve outcomes and can carry its own risks, such as blood clots and muscle weakness.
Moderate to Severe Cases
- More frequent prenatal appointments and ultrasounds.
- Hospital admission for close monitoring, medicines to help delay premature labor when appropriate, corticosteroid injections to help the baby’s lungs mature if preterm delivery is anticipated, and blood transfusions if significant blood loss occurs.
- Emergency cesarean delivery for heavy or uncontrolled bleeding, or other signs of danger to the mother or baby.
- Admittance to the hospital’s labor and delivery unit for vaginal bleeding after 20 weeks.
- C-section delivery at 36 weeks for extreme blood loss or risk to maternal or fetal health.
Planned Delivery
- Vaginal delivery if placenta previa resolves, but a C-section delivery is planned if it doesn’t resolve.
- Planned C-section delivery between 36 and 37 weeks, even for those with no bleeding, to reduce the risk of sudden bleeding during labor.
- If delivery is planned before 37 weeks, corticosteroids may be given to help the baby’s lungs develop.
- Do’s
- Seek emergency medical care if vaginal bleeding or contractions occur.
- Follow the healthcare provider’s recommendations for treatment and management. Get more frequent prenatal appointments and ultrasounds if recommended.
- Don’ts:
- Avoid sexual activity, moderate or strenuous exercise, heavy lifting, and standing for long periods of time to lower the risk of possible bleeding2.
Prevention of Placenta Previa
Placenta previa cannot always be prevented. Many of its risk factors, such as a previous cesarean delivery, prior uterine surgery, or advancing maternal age, are not within a person’s control. However, the following steps may help lower your risk where possible and support a safer pregnancy:
Dos
- Seek medical care promptly if you experience any symptoms of placenta previa.
- Work closely with your healthcare team to manage placenta previa and reduce the risk of complications for both you and your baby.
- If you have risk factors for placenta previa, follow your healthcare provider’s recommendations for additional monitoring during pregnancy.
Don’ts
- Do not smoke or use cocaine, as these substances increase the risk of placenta previa. Avoiding them can help lower your risk2.
Complications of Placenta Previa
Placenta previa poses risks for both the mother and the baby. Here are some potential complications:
For the Mother
- Severe bleeding: This can happen during pregnancy, labour, or delivery and can be life-threatening.
- Early birth: If bleeding is severe, an emergency C-section may be necessary before the baby is full-term.
- Blood loss: Losing too much blood can lead to anaemia, low blood pressure, pale skin, or shortness of breath.
- Placenta accreta: The placenta can grow too deeply into the uterine wall, resulting in severe bleeding after delivery.
- Placental abruption: The placenta separates from the uterus before the baby is born, reducing the baby’s supply of oxygen and nutrients.
For the Baby
- Premature birth: If bleeding is severe, an emergency C-section may result in the baby being born too early.
- Low birth weight: Low birth weight can lead to trouble staying warm and poor weight gain.
- Respiratory issues: Underdeveloped lungs can make breathing more difficult.
Additionally, placenta previa can lead to haemorrhage, emergency C-sections, and placenta accreta spectrum, which is a group of conditions where the placenta grows into or through the wall of the uterus, increasing the risk of bleeding during pregnancy or delivery. Close monitoring by healthcare providers can help reduce the risk of these complications2.
When to See a Doctor?
- Any vaginal bleeding during the second or third trimester of pregnancy should be immediately reported to your healthcare provider.
- Even if the bleeding appears to be mild or stops after a short period, it is still essential to seek medical evaluation to rule out any serious underlying conditions.
- If the bleeding is heavy or accompanied by severe cramps or you are feeling unwell, seek emergency medical care right away.
- Do not delay seeking medical attention as early intervention can be crucial for ensuring a healthy pregnancy and delivery2.
Also Read: Are Blood Clots During Your Period Normal? Causes and Treatment Options
Conclusion
Placenta previa is a serious but manageable pregnancy complication in which the placenta partially or completely covers the cervix. While it cannot always be prevented, most cases are identified through routine ultrasound and can be safely managed with close monitoring, activity modification, and, when needed, a planned cesarean delivery, typically between 36 and 37 weeks. Prompt reporting of any vaginal bleeding, regular prenatal care, and open communication with your healthcare provider remain the most important steps toward a safe delivery for both mother and baby.
Frequently Asked Questions (FAQs)
Does placenta previa always require a C-section?In most cases, a C-section is necessary for the safe delivery of the baby.
Is it possible for the placenta to move away from the cervix?In some cases, the placenta can move away from the cervix as the uterus grows.
Is placenta previa very common?Every 1 in 200 pregnancies, on average, can show placenta previa.
Is placenta previa hereditary?No, there is no evidence to suggest that placenta previa is hereditary.
Is it possible to have placenta previa and not experience any symptoms?Yes, some women may have placenta previa without experiencing any symptoms.
References
- ‘Placenta praevia’ [online], in The Merck Manual of Diagnosis and Therapy, Section 18, Gynaecology and Obstetrics, Chapter 252, Abnormalities of Pregnancy. Eds R. Berkow, M. Beers, A. Fletcher & R. Bogin. Merck & Co. Inc., Whitehouse Station, NJ, USA. Available from: https://www.merckmanuals.com/professional/gynecology-and-obstetrics/abnormalities-of-pregnancy/placenta-previa
- Placenta previa: Symptoms, causes & treatments [Internet]. Cleveland Clinic. Available from: https://my.clevelandclinic.org/health/diseases/24211-placenta-previa
- Anderson-Bagga FM, Sze A. Placenta Previa.In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated 2022 Jun 21-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539818/
- Placenta previa: Medlineplus medical encyclopedia [Internet]. MedlinePlus. U.S. National Library of Medicine; Available from: https://medlineplus.gov/ency/article/000900.htm
- Rowe T. Placenta previa. Journal of Obstetrics and Gynaecology Canada: JOGC= Journal D’obstetrique et Gynecologie du Canada: JOGC. 2014 Aug 1;36(8):667-8. Available from: https://www.jogc.com/article/S1701-2163(15)30503-X/fulltext
- Zlatnik MG, Little SE, Kohli P, Kaimal AJ, Stotland NE, Caughey AB. When should women with placenta previa be delivered? A decision analysis. The Journal of reproductive medicine. 2010 Sep;55(9-10):373. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6633882/
- Taylor VM, Peacock S, Kramer MD, Vaughan TL. Increased risk of placenta previa among women of Asian origin. Obstet Gynecol. 1995;86(5):805-808. doi:10.1016/0029-7844(95)00262-P. Available at: https://www.sciencedirect.com/science/article/abs/pii/002978449500262P
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
 1
1 












































Comments