Cholesterol is a wax-like, fatty substance found in the body essential for building cells, producing hormones, and supporting digestion. There are different types of cholesterol such as low-density lipoprotein (LDL), high-density lipoprotein (HDL), and very low-density lipoprotein (VLDL)1.
LDL cholesterol is generally referred to as bad cholesterol because when it is in excess, it can accumulate in the arteries, increasing the risk of heart disease2. Since high LDL cholesterol usually does not cause noticeable symptoms in the early stages3, many people may be unaware of their condition until difficulties arise.
This article will guide you about the possible effects of high LDL cholesterol as well as its causes, risk factors and management strategies.
LDL stands for low-density lipoprotein. The body needs some LDL cholesterol for normal functioning. However, LDL is known as bad cholesterol because when it is inexcess it can accumulate within the arteries and form fatty deposits known as plaques (atherosclerosis) 1,2. As plaque accumulates, the arteries narrow and harden, decreasing blood flow to vital organs including the heart and brain. If a plaque breaks open, it may form a blood clot that can completely block blood flow. This may lead to:
On the other hand, HDL cholesterol is known as good cholesterol because it helps remove excess cholesterol from the bloodstream1.
LDL cholesterol levels are measured through a fasting blood test called lipid profile and are usually expressed in milligrams per decilitre (mg/dL). Here is a table which shows different ranges of LDL cholesterol.
| LDL Cholesterol Level | Category |
| Less than 100 mg/dL | Optimal |
| 100-129 mg/dL | Near optimal (above optimal) |
| 130-159 mg/dL | Borderline high |
| 160-189 mg/dL | High |
| 190 mg/dL and above | Very high |
Note: LDL cholesterol levels can vary slightly based on the laboratory, age, medical history, and personal risk factors. Always consult a doctor for proper interpretation of your lipid profile results and personalised medical advice.

Several factors can increase LDL cholesterol levels. Here are some factors that explain what causes high LDL cholesterol levels.
Note: Reasons for high LDL cholesterol can vary among individuals. Therefore, proper diagnosis is important.
High LDL cholesterol symptoms are rarely apparent in the early stages. Many people find out only after a regular blood test or when issues arise. Severe or long-standing high LDL cholesterol can sometimes cause symptoms due to restricted blood flow causing severe conditions3,4,5. These may include the following:
Note: These symptoms typically reflect complications from long-term plaque buildup, not high LDL itself. Consult a doctor for proper evaluation and diagnosis.
The following are some risk factors that can contribute to high LDL Cholesterol:
Your doctor might suggest a lipid profile test to measure the LDL cholesterol levels. This test measures:
From this test results, high LDL cholesterol means there is an increased risk of artery clogs which can cause heart disease and other complications2.
The doctors may recommend this test:
Note: Lipid profile results should always be interpreted by a doctor along with your medical history, symptoms, and overall health condition.
As a part of high LDL cholesterol treatment, your doctor might prescribe certain medications if the cholesterol levels do not come down with lifestyle changes alone2. There are different types of medicines your doctor might give; these include the following:
Note: These medications should only be taken as prescribed by a doctor. The type of medication and dosage may differ depending on the patient’s cholesterol levels, overall health, and medical history. Do not start, stop, or change any medicine without first consulting a doctor.
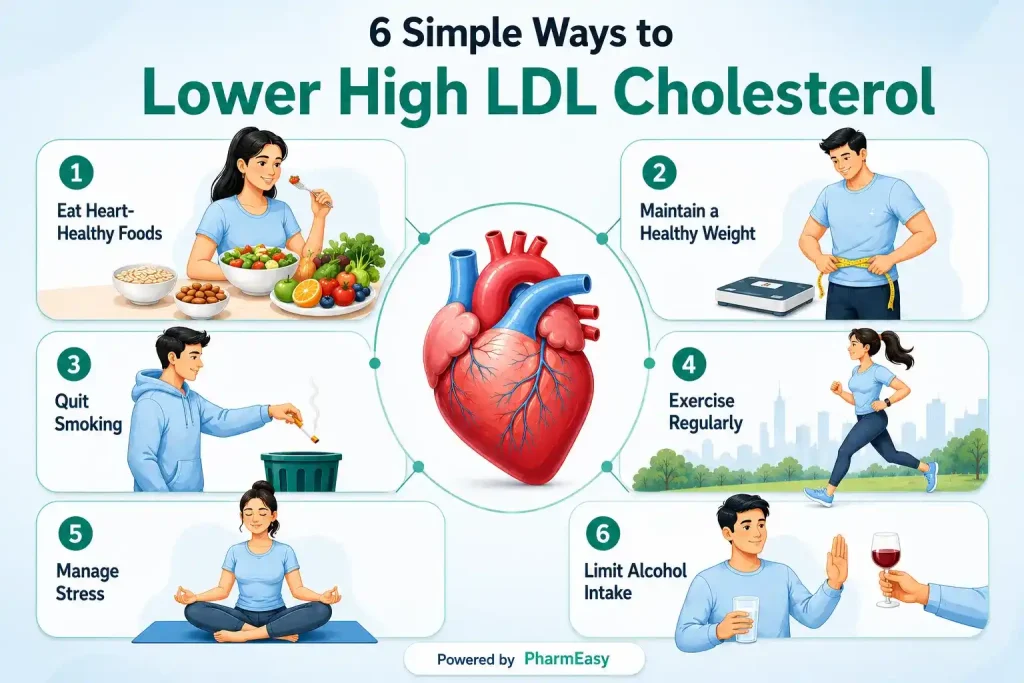
High LDL cholesterol can often be reduced through healthy lifestyle changes. The following are some simple ways by which you can help manage your LDL levels along with a proper medical treatment:
Note: Lifestyle changes may assist manage high LDL cholesterol, but their effectiveness may differ from person to person. Some people may also need medications or other medical treatments depending on their cholesterol levels, overall health, and risk of heart disease. Always seek the opinion of a doctor for an accurate diagnosis, treatment, and individualised care.
Certain foods can help naturally reduce LDL cholesterol levels. These include the following:
Note: This information is for educational purposes only and should not be considered medical advice. Diet alone may not be sufficient to control high LDL cholesterol in all cases. It is important to see a doctor or a dietician for an accurate treatment and dietary recommendations.
Also Read: High Alkaline Phosphatase Levels: Causes, Symptoms & Treatment
If left untreated, high LDL cholesterol can lead to serious health problems, such as:
Hence, it is important to check your cholesterol levels as a part of routine checkup, as high LDL levels can cause severe blockage of the arteries, thereby contributing to life-threatening if not treated on priority.
You should consult a doctor if you have a family history of high cholesterol or heart disease, are experiencing symptoms such as chest pain, shortness of breath, or leg pain, or have conditions such as diabetes, obesity, or high blood pressure. If your cholesterol readings continue to rise even after lifestyle adjustments, it is important to get medical care.
Also Read: High Triglycerides: Causes, Symptoms, Diagnosis & How to Reduce It
High LDL cholesterol is a frequent health issue with no early warning signs. If not addressed, it can raise the risk of heart disease and stroke. Healthy habits including eating nutritious foods, exercising regularly, maintaining a healthy weight, and following medical advice can all help lower LDL cholesterol and safeguard heart health.
Yes, high LDL cholesterol can be reduced and controlled by adopting good lifestyle habits such as a balanced diet, frequent exercise, weight management, and quitting smoking. In some cases, doctors may also recommend medications to help lower LDL cholesterol and lower the risk of heart disease2.
Although it is difficult to reduce LDL levels in seven days, a healthy lifestyle can slowly help reduce it. You can start by avoiding fried and processed foods, eating more fruits, vegetables, oats, and nuts, and exercising regularly. Quitting smoking, reducing alcohol intake, and staying physically active can also help improve cholesterol levels quickly1,2,3.
Drinks such as green tea, oat-based drinks, low-fat milk, and smoothies made with fruits and vegetables may help lower cholesterol levels. Limiting sugary drinks and alcohol can also support better heart health2,13,14.
For most healthy people, eating 1–2 eggs a day is generally considered safe and may not significantly raise cholesterol levels. However, people with high cholesterol, diabetes, or heart disease should consult a doctor about the right amount for their diet15.
The LDL level by age is given below:
Children younger than 19: < 110 mg/dL16
Adults: < 100 mg/dL (optimal)2
However,for people with certain heart conditions, doctors may recommend keeping LDL cholesterol at even lower levels to reduce the risk of heart-related complications.
1. Cholesterol Med. 2025. doi:https://medlineplus.gov/cholesterol.html
2. LDL: The “Bad” Cholesterol. 2024. doi:https://medlineplus.gov/ldlthebadcholesterol.html
3. Cholesterol. 2024. doi:https://www.healthdirect.gov.au/cholesterol
4. Peripheral Arterial Disease. 2025. doi:https://medlineplus.gov/peripheralarterialdisease.html
5. Stroke. 2025. doi:https://medlineplus.gov/stroke.html
6. Herink MC. Medication Induced Changes in Lipids and Lipoproteins. 2025. doi:https://www.ncbi.nlm.nih.gov/books/NBK326739/
7. Duntas LH. Thyroid Disease and Lipids. Thyroid. 2002;12(4):287-293. doi:10.1089/10507250252949405 https://pubmed.ncbi.nlm.nih.gov/12034052/
8. Lipid profile test. 2024. doi:https://medlineplus.gov/ency/article/007812.htm
9. Cholesterol-Lowering Medicines. 2024. doi:https://www.cdc.gov/cholesterol/treatment/cholesterol-lowering-medicines.html
10. Ray KK, Ference BA, Séverin T, et al. World Heart Federation Cholesterol Roadmap 2022. gh. 2022;17(1):75. doi:10.5334/gh.1154 https://pubmed.ncbi.nlm.nih.gov/36382159/
11. Heart-Healthy Living. 2022. doi:https://www.nhlbi.nih.gov/health/heart-healthy-living/healthy-foods
12. Soybeans and soy foods. 2026. doi:https://www.betterhealth.vic.gov.au/health/healthyliving/soybeans
13. High Cholesterol = High Kidney Disease Ri. 2014. doi:https://www.kidney.org/news-stories/high-cholesterol-high-kidney-disease-risk
14. Xu R, Yang K, Li S, Dai M, Chen G. Effect of green tea consumption on blood lipids: a systematic review and meta-analysis of randomized controlled trials. Nutr J. 2020;19(1):48. doi:10.1186/s12937-020-00557-5 https://pubmed.ncbi.nlm.nih.gov/32434539/
15. Shin JY, Xun P, Nakamura Y, He K. Egg consumption in relation to risk of cardiovascular disease and diabetes: a systematic review and meta-analysis. The American Journal of Clinical Nutrition. 2013;98(1):146-159. doi:10.3945/ajcn.112.051318 https://pubmed.ncbi.nlm.nih.gov/23676423/
16. High Cholesterol in Children and Teens. 2024. doi:https://medlineplus.gov/highcholesterolinchildrenandteens.html
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.


You may be confused if your blood test results show high triglyceride levels, especially if you have no visible symptoms. Triglycerides are a form of fat found in the blood that your body uses for energy1. However, when their levels rise too high, they might raise the risk of serious health issues such as heart disease, stroke, fatty liver disease, and pancreatitis2.
The good news is that high triglycerides can often be managed with the right lifestyle changes, healthy eating habits, and timely medical care. In this blog, you will learn what high triglycerides mean, their causes and symptoms, how they are diagnosed, and effective ways to reduce them naturally and medically.
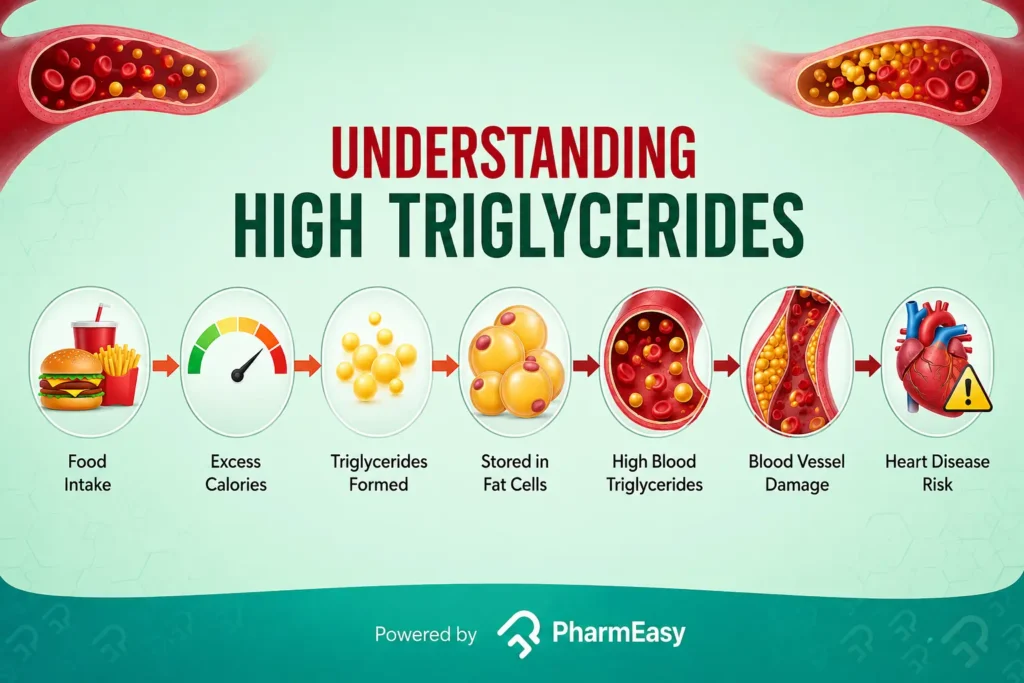
High triglycerides means that there is an excess amount of triglycerides, a type of fat (lipid), circulating in your blood.
Our bodies use calories for functioning and physical activity, which are supplied from the food we eat. Excess calories that are not utilised by the body get converted into triglycerides, which are not needed immediately. These triglycerides are stored in fat cells and used for energy when required1.
Triglycerides are important for normal body function, but having too much of them in the blood can become harmful. High triglyceride levels are frequently associated with unhealthy lifestyle practices such as consuming too much sweet or fatty food, lack of physical activity, smoking, consuming excessive alcohol, etc2. They can also occur due to conditions like diabetes, thyroid disorders, kidney disease, or due to certain medications1.
In most cases, high triglycerides do not cause noticeable symptoms2, which is why many people discover them only during a routine blood test called a lipid profile. When triglyceride levels remain high for a long time, fatty deposits can build up in blood vessels, making it harder for blood to flow properly (atherosclerosis). This increases the risk of heart-related diseases and other complications3. Very high triglyceride levels can also affect the pancreas, leading to a painful condition called pancreatitis2.
Since symptoms are often absent, regular health check-ups and lipid profile tests are important for early detection.
High triglycerides can be caused by an unhealthy lifestyle, certain medical problems, drugs, or genetics. Common causes include:
Certain medications such as corticosteroids, hormonal pills (oestrogen), antivirals (ritonavir), antipsychotics, water pills (diuretics), BP medications (beta blockers) can increase triglycerides in the body2,10.
Some genetic disorders can also cause high triglyceride levels. Examples: Familial hypertriglyceridemia and combined hyperlipidaemia3.
Identifying the reasons for high triglycerides are important for choosing the right treatment and lifestyle changes to lower triglyceride levels effectively.
Triglyceride levels are measured through a blood test known as a lipid profile. These levels help doctors determine how much fat is in your blood and whether it raises your risk of heart disease and other health issues.
The following is a table which shows the ranges of triglycerides1:
| Category | Triglyceride Ranges (mg/dL) |
| Normal | < 150 |
| Borderline high | 150 – 199 |
| High | 200 – 499 |
| Very high | 500 and above |
If you have normal triglycerides, it may suggest your body is successfully consuming and storing fats for energy without allowing excess fat to accumulate in the bloodstream. People who have normal triglyceride levels are less likely to have heart disease, stroke, or pancreatitis, especially if their other cholesterol levels are also within healthy range11.
High triglyceride levels imply that there is too much fat circulating in the blood. This usually occurs when the body consumes or retains more calories than it burns. Over time, extra fats can harden or restrict blood vessels, increasing the risk of cardiovascular disease2.
Triglyceride levels above 500 mg/dL can increase the risk of pancreatic inflammation (pancreatitis), resulting in severe stomach pain. Very high levels may also alter blood vessels in the eyes, and cause skin changes on the chest, back, arms, or legs. Extremely high triglyceride levels (above 1,500 mg/dL) can sometimes stop the body from properly breaking down fats, a very dangerous condition called multifactorial chylomicronaemia syndrome2.
Therefore, checking triglyceride levels regularly is important to identify potential health risks early. People with diabetes, obesity, heart disease, thyroid disorders, or a family history of lipid disorders may need more frequent monitoring2.
Note: Triglyceride or lipid profile levels should be interpreted by a qualified doctor, as the results might vary depending on age, medical history, medications, and other personal factors.
High triglyceride levels are detected with a simple blood test known as a lipid profile, which analyses the amount of fats (lipids) in the blood, including triglycerides, cholesterol (LDL, HDL), and total cholesterol. This test allows doctors to determine your risk of heart disease and other problems12.
Your doctor will collect a simple blood sample, usually from an arm vein, for the test. It is a short, very minimally invasive process. The obtained sample is then analysed in a laboratory to identify the concentration of triglycerides in the bloodstream, as well as other lipid parameters12.
For accurate triglyceride results, fasting is generally recommended:
Note: Taking a test without fasting can show variations in values of triglycerides and other lipids. Talk to your doctor if you are taking any medications or supplements, as they can also interfere with the result. Also, do not stop any medications without your doctor’s permission12.
Your doctor might suggest a lipid profile test in the following situations:
Your doctor might suggest taking the test in the morning following an overnight fast, making it easier to meet the fasting requirement and ensuring consistent and reliable findings15.
High triglyceride levels are addressed based on their severity and the individual’s overall risk of heart disease or pancreatitis. Doctors may give drugs to help lower triglycerides and avoid problems. Common medications include the following:
Doctors may also address conditions like diabetes or thyroid issues that trigger excessive triglyceride levels. Managing these conditions helps improve overall lipid levels2.
Note: The information provided in this section is for general educational purposes only and is not intended to substitute professional medical advice, diagnosis, or treatment.

A healthy diet plays an important role in managing high triglyceride levels. Certain foods can help improve fat metabolism, support heart health, and reduce excess triglycerides in the blood. The following are few among them:

High triglyceride levels can be worsened by certain foods, so it is important to limit or avoid them to help maintain better blood lipid control. Here are few among them:
High triglyceride levels can typically be reduced with easy lifestyle adjustments that enhance fat management and general heart health. These include the following:
You should consult a doctor if:
Early diagnosis and treatment may help avoid serious complications and improve long-term health.
Also Read: 10 Healthy Fat Foods That You Should Be Eating!
High triglycerides are common and can be managed. They usually don’t show symptoms early, but if left untreated, they can increase the risk of heart disease and other health problems. Regular blood tests, healthy eating, exercise, and proper medical care can help control triglyceride levels. Making early lifestyle changes and getting timely treatment can help protect your heart and overall health.
Also Read: Low HDL (Good) Cholesterol: Causes, Symptoms & How to Increase It
No, triglycerides are not checked in a complete blood count (CBC) test. They are measured in a separate test called a lipid profile12.
Triglycerides are made up of fatty acids that can be either saturated or unsaturated. Unsaturated fats are generally considered to be a healthier option21.
High triglycerides mainly affect the blood vessels and heart. These increasing the risk of atherosclerosis (plaque buildup) in the arteries of heart and can lead to heart disease. In very severe cases, they can also affect the pancreas, leading to a condition called pancreatitis2,3.
Yes, chronic stress can contribute to high triglyceride levels. It can trigger hormonal changes that increase fat production and also lead to unhealthy habits like overeating or lack of exercise, which raise triglycerides7.
High triglycerides do not directly cause diabetes. However, they are often linked with metabolic syndrome (which includes insulin resistance- low sensitivity of tissues to insulin, decreasing blood sugar utilisation by the body) that increases the risk of developing type 2 diabetes3.
1. Triglycerides med. 2025. doi:https://medlineplus.gov/triglycerides.html
2. High Blood Triglycerides. 2025. doi:https://www.nhlbi.nih.gov/health/high-blood-triglycerides
3. Triglycerides. doi:https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/triglycerides
4. Eruptive xanthomatosis. 2024. doi:https://medlineplus.gov/ency/article/007746.htm
5. Peripheral Neuropathy. doi:https://www.niddk.nih.gov/health-information/diabetes/overview/preventing-problems/nerve-damage-diabetic-neuropathies/peripheral-neuropathy
6. Pancreatitis. 2024. doi:https://medlineplus.gov/pancreatitis.html
7. Anni NS, Jung SJ, Shim JS, Jeon YW, Lee GB, Kim HC. Stressful life events and serum triglyceride levels: the Cardiovascular and Metabolic Diseases Etiology Research Center cohort in Korea. Epidemiol Health. 2021;43:e2021042. doi:10.4178/epih.e2021042 https://pubmed.ncbi.nlm.nih.gov/34126706/
8. Smellie WSA. Hypertriglyceridaemia in diabetes. BMJ. 2006;333(7581):1257-1260. doi:10.1136/bmj.39043.398738.DE https://pmc.ncbi.nlm.nih.gov/articles/PMC1702429/
9. Pearce EN. Hypothyroidism and dyslipidemia: Modern concepts and approaches. Curr Cardiol Rep. 2004;6(6):451-456. doi:10.1007/s11886-004-0054-3 https://pubmed.ncbi.nlm.nih.gov/15485607/
10. Herink MC. Medication Induced Changes in Lipids and Lipoproteins. 2025. doi:https://www.ncbi.nlm.nih.gov/books/NBK326739/
11. In brief: Triglycerides. 2025. doi:https://www.ncbi.nlm.nih.gov/books/NBK618443/
12. Lipid profile test. 2024. doi:https://medlineplus.gov/ency/article/007812.htm
13. Fasting for a Blood Test. 2025. doi:https://medlineplus.gov/lab-tests/fasting-for-a-blood-test/
14. Testing for Cholesterol. 2024. doi:https://www.cdc.gov/cholesterol/testing/index.html
15. Nigam PK. Serum Lipid Profile: Fasting or Non-fasting? Ind J Clin Biochem. 2011;26(1):96-97. doi:10.1007/s12291-010-0095-x https://pubmed.ncbi.nlm.nih.gov/22211025/
16. Fiber: The Carb That Helps You Manage Diabetes. 2024. doi:https://www.cdc.gov/diabetes/healthy-eating/fiber-helps-diabetes.html
17. Nurzyńska-Wierdak R. Green Leafy Vegetables (GLVs) as Nutritional and Preventive Agents Supporting Metabolism. Metabolites. 2025;15(8):502. doi:10.3390/metabo15080502 https://pubmed.ncbi.nlm.nih.gov/40863121/
18. Guasch-Ferré M, Tessier AJ, Petersen KS, et al. Effects of Nut Consumption on Blood Lipids and Lipoproteins: A Comprehensive Literature Update. Nutrients. 2023;15(3):596. doi:10.3390/nu15030596 https://pubmed.ncbi.nlm.nih.gov/36771303/
19. Dietary advice for management of high triglycerides. 2024. doi:https://www.cuh.nhs.uk/patient-information/dietary-advice-for-management-of-high-triglycerides/
20. Warning signs and symptoms of heart disease. 2024. doi:https://medlineplus.gov/ency/patientinstructions/000775.htm
21. Jadhav HB, Annapure US. Triglycerides of medium-chain fatty acids: a concise review. J Food Sci Technol. 2023;60(8):2143-2152. doi:10.1007/s13197-022-05499w https://pubmed.ncbi.nlm.nih.gov/35761969/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Planning for a baby is often filled with hope, but when things don’t go as expected, it can be confusing and stressful for both parents. What many people don’t realise is that fertility challenges are not limited to women; male factors can also contribute to them.
Male infertility refers to a man’s inability to achieve a pregnancy with his partner. It is a common but often overlooked factor in infertility. The good news is that in many cases, this is manageable with proper medical guidance and care1.
In this blog, we will cover male infertility causes, symptoms, diagnosis, and management options for male infertility, along with when to seek medical advice.
Infertility is not only a female issue. Male factors play a role in many cases. In fact, around one-third of infertility cases are due to male-related problems.
Male infertility refers to difficulty in achieving pregnancy with their partner even after having regular, unprotected intercourse for one year2.
The types of male infertility can be broadly classified as follows3:
Male infertility can occur due to problems in different parts of the male reproductive system (including the testes, sperm-carrying tubes, glands, and hormones involved in sperm production). Common male infertility causes include3:
These involve problems with the hormones that control sperm production. Hormones from the testicles and the pituitary and hypothalamus areas of the brain control sperm production. So, any imbalance in these hormones can affect fertility.
These can affect the production and quality of sperm:
These involve problems with movement of sperm through the reproductive system and their delivery during ejaculation. These may be caused by a blockage in the reproductive tract due to infections, injuries, or damage to the genital tract.
Note: In some men, semen analysis may be abnormal, but no clear cause of infertility is identified despite detailed evaluation. This is known as idiopathic male infertility and accounts for around 30% of male infertility cases4.
In most cases, men may not have any obvious symptoms of infertility, and the most common sign is difficulty in achieving pregnancy despite regular, unprotected intercourse. However, some male infertility symptoms may point to underlying issues, for example:
Certain factors can increase the risk of male infertility by affecting sperm production, quality, or delivery. Common risk factors include:
Infertility in men is diagnosed through a combination of medical history, physical examination, and laboratory tests. These include1,10:
The doctor will ask about health history, lifestyle, past illnesses, medications, and sexual history. A physical exam may be done to check the testicles and reproductive organs for any visible problems.
This is a key test for evaluating male infertility.
These tests check hormones like testosterone, luteinising hormone (LH), prolactin, and follicle-stimulating hormone (FSH) to see if there is a hormonal issue affecting sperm production. Blood tests for male infertility may also help identify infections, genetic conditions, vitamin deficiencies, and underlying health issues that can affect male reproductive health and fertility. Your doctor may also suggest blood tests that include many important parameters that can check a male’s reproductive health.
Tests like scrotal ultrasound help detect problems such as varicocele or blockages in the reproductive tract.
These may include:
The management of male infertility depends on its cause. In some cases, pregnancy may still occur naturally, but medical care can improve the chances. Your doctor may suggest and prescribe one of the following options for male infertility treatment1:
In cases of hormonal imbalance, therapies using hormones like human chorionic gonadotropin (hCG), FSH, or other medications may help improve sperm production, especially in specific conditions.
If male infertility treatment options like medications do not work, ARTs such as the following may be used to help achieve pregnancy:
Surgery may be needed to fix physical problems such as a varicocele or blockages in the reproductive tract. These procedures may help improve sperm flow and fertility in some men.
Male fertility is closely linked to lifestyle and overall health. So, making the right changes can help improve sperm quality and support reproductive health. Some options include1,11:

Eating foods rich in nutrients like omega-3 fatty acids, vitamins (C, E), zinc, and folate supports sperm production and protects sperm from damage. Therefore, following a diet rich in fruits, vegetables, whole grains, and healthy fats could be beneficial.

Both obesity and being underweight can affect hormones and reduce sperm production. So, trying to maintain an ideal weight may help improve fertility.

Moderate physical activity improves hormone levels and sperm quality, while too little or too much exercise may have negative effects.

Smoking, excessive alcohol, and other recreational drugs (like marijuana) may affect sperm health. Thus, quitting or reducing their use may improve fertility over time.

Chronic stress can affect hormones and lower testosterone, impacting sperm production. So, if you feel stressed, management techniques like meditation or therapy might help.

Poor sleep or irregular sleep patterns can reduce sperm quality and affect fertility. Thus, getting proper sleep is important for hormone balance.

Excess heat (like hot tubs or tight clothing) and exposure to toxins, chemicals, or radiation might harm sperm production. So, you should try to avoid them as much as possible.

Regular intercourse, especially around ovulation, can improve chances of conception. Also, some lubricants (such as the artificial ones) may affect sperm movement and should be chosen carefully.
Also Read: HIV Cure: Is it possible? Know the Symptoms and Treatment Options
Knowing when to seek medical help can improve the chances of early diagnosis and management. You should consider seeing a doctor if you have1,5,6,7,11:
Note: Couples trying to conceive are generally advised to have regular intercourse every 2 to 3 days, undergo evaluation of both partners, and understand that improvements in sperm health may take around 3 months12.
Also Read: Varicocele – Symptoms, Causes, Home Remedies
Male infertility is a common yet often overlooked condition that can significantly affect a couple’s ability to conceive. Reasons for male infertility include sperm-related issues, hormonal imbalances, lifestyle influences, and underlying medical conditions.
The reassuring part is that many cases are manageable with the right diagnosis and care. From lifestyle changes and medications to advanced male infertility treatments like IVF and ICSI, there are multiple options available to improve the chances of conception.
Apart from this, seeking timely medical advice, making informed lifestyle choices, and addressing both physical and emotional aspects can make a meaningful difference. With the right support and approach, many couples can successfully achieve their goal of parenthood.
The main sign is difficulty in achieving pregnancy despite regular, unprotected intercourse for a year. Most men do not have obvious symptoms, so a semen analysis test is needed to confirm1.
Yes, smoking could lower sperm count, reduce sperm motility, and damage sperm quality13.Therefore, quitting might help improve fertility over time.
Heavy alcohol use can reduce testosterone levels and affect sperm production14. Occasional or moderate intake may have less impact, but excess drinking should be avoided.
Vaping may affect sperm quality due to the chemicals and nicotine in it15. Research is still growing, but it is considered potentially harmful to fertility, so precautions should be taken.
Not always. Some male infertility causes are temporary and manageable, while others may be long-term. It depends on the underlying cause. Thus, if there are concerns, you should always consult a doctor.
In some cases, genetic conditions or chromosomal abnormalities (such as Kallmann syndrome, Klinefelter syndrome, Young syndrome, etc.) could affect sperm production and function1.
Male infertility may be reversible in some cases, especially when caused by lifestyle factors, infections, or hormonal issues. However, not all cases might be fully reversed. Your doctor will be able to provide you with a better insight into this.
There is no strong proof or evidence that cell phones cause male infertility; however, long-term exposure to heat and radiation (like keeping phones in pockets) may affect sperm quality9. So, limiting exposure is a good precaution.
High caffeine and additives in energy drinks may affect sperm quality if consumed in excess16. Occasional intake may be fine, but overuse should be avoided.
1. Leslie SW, Soon-Sutton TL, Khan MA. Male Infertility. In: StatPearls. StatPearls Publishing; 2026. Accessed April 30, 2026. http://www.ncbi.nlm.nih.gov/books/NBK562258/
2. Male Infertility. Accessed April 30, 2026. https://medlineplus.gov/maleinfertility.html
3. Infertility. Accessed April 30, 2026. https://www.who.int/news-room/fact-sheets/detail/infertility
4. Corsini C, Boeri L, Candela L, et al. Is There a Relevant Clinical Impact in Differentiating Idiopathic versus Unexplained Male Infertility? World J Mens Health. 2023;41(2):354-362. doi:10.5534/wjmh.220069 https://pmc.ncbi.nlm.nih.gov/articles/PMC10042653/
5. Sexual Problems in Men. Accessed April 30, 2026. https://medlineplus.gov/sexualproblemsinmen.html
6. Paick S, Choi WS. Varicocele and Testicular Pain: A Review. World J Mens Health. 2019;37(1):4-11. doi:10.5534/wjmh.170010 https://pubmed.ncbi.nlm.nih.gov/29774668/
7. Infertility: MedlinePlus Medical Encyclopedia. Accessed April 30, 2026. https://medlineplus.gov/ency/article/001191.htm
8. El Osta R, Almont T, Diligent C, Hubert N, Eschwège P, Hubert J. Anabolic steroids abuse and male infertility. Basic Clin Androl. 2016;26:2. doi:10.1186/s12610-016-0029-4 https://pmc.ncbi.nlm.nih.gov/articles/PMC4744441/
9. Mortazavi SAR, Taeb S, Mortazavi SMJ, et al. The Fundamental Reasons Why Laptop Computers should not be Used on Your Lap. J Biomed Phys Eng. 2016;6(4):279-284. https://pmc.ncbi.nlm.nih.gov/articles/PMC5219578/
10. Sunder M, Leslie SW. Semen Analysis. In: StatPearls. StatPearls Publishing; 2026. Accessed May 4, 2026. http://www.ncbi.nlm.nih.gov/books/NBK564369/
11. Bocu K, Boeri L, Mahmutoglu AM, Vogiatzi P. Can lifestyle changes significantly improve male fertility: A narrative review? Arab J Urol Int J. 23(3):190-200. doi:10.1080/20905998.2024.2421626 https://pmc.ncbi.nlm.nih.gov/articles/PMC12308861/
12. Infertility-Prevention-and-Management-Guideline-.pdf. Accessed May 4, 2026. https://moh.gov.bt/wp-content/uploads/2025/02/Infertility-Prevention-and-Management-Guideline-.pdf?
13. The Effects of Cigarette Smoking on Male Fertility – PMC. Accessed April 30, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC4639396/
14. Alcohol’s Effects on Male Reproduction – PMC. Accessed April 30, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC6761906/
15. An Overview of E-Cigarette Impact on Reproductive Health – PMC. Accessed April 30, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC10053939/
16. Ricci E, Viganò P, Cipriani S, et al. Coffee and caffeine intake and male infertility: a systematic review. Nutr J. 2017;16:37. doi:10.1186/s12937-017-0257-2 https://pubmed.ncbi.nlm.nih.gov/28646871/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
A fall or accident can instantly cause a broken bone, affecting your mobility and daily life. Bone fractures are the most common orthopaedic injuries, occurring when a bone cracks or breaks due to sudden impact, trauma, or weak bone structure1. Early recognition of fractures is important because timely treatment might help avoid severe complications like deformity or long-term pain.
Fractures can occur irrespective of age, and they can vary from a simple hairline fracture to complete breaks. The major causes of bone fractures are falls, sports injuries, road accidents, osteoporosis, and repetitive stress on the bone. Maintaining bone strength through a proper diet and understanding other preventive measures might reduce the risk of bone fractures and promote long-term skeletal health1.
In this article, we will discuss bone fractures, their types, symptoms, treatment options, etc.
As mentioned earlier, a bone fracture is a condition in which a bone cracks or breaks completely1. This may occur due to conditions like falls, road accidents, or sports injuries when the bone is subjected to pressure that it cannot withstand, causing it to split or break2. In some cases, bones weakened by conditions like osteoporosis or repeated stress are more likely to fracture, even with minor pressure. Bone fractures can range from a thin crack to a full break where the bone splits into multiple pieces depending on the force it is subjected to. For example, in high impact situations, such as in a car accident or gunshot injury, the bone can break into multiple pieces1.
Although bones are strong, they may fracture under certain conditions, such as:
A fracture is called a closed fracture when the bone breaks but does not pierce the skin, making it less exposed to infection. Open fracture occurs when the broken bone breaks through the skin, creating a wound, making it prone to infection3. Open fractures require immediate medical attention due to high chances of complications.
The symptoms of bone fracture usually depend on the type of fracture and severity. Some common bone fracture symptoms include:
There are various types of bone fractures based on the affected part of the body and their cause. All fractures require immediate medical attention; avoid relying solely on home remedies. Provide only quick first aid if needed and take the patient to the nearest hospital as soon as possible. The types of bone fractures, their causes, and basic first aid measures are as follows.

This is a fracture where the bone breaks but does not pierce the skin3. The injury is internal, and the risk of infection is lower compared to open fractures. Can occur from falls, minor accidents, or direct impact where the force is enough to break the bone but not the skin.
First aid for the fracture:

In this type of fracture, the broken bone sticks out through the skin or creates a wound that reaches the bone. The risk of bleeding and infection is very high3. It is commonly caused by severe trauma such as road accidents, falls from height, or high-impact injuries4.
First aid for the fracture:

Greenstick fractures usually occur in children as their bones are more flexible than adults. This is a partial thickness fracture, in which the bone partially breaks on one side while the other side stays intact. It can occur after a fall and from accidents, sports injuries, or being hit. Malnutrition, in particular, vitamin D deficiency, increases the likelihood of Greenstick fractures5.
First aid for the fracture:

In this type of fracture, the bone breaks into three or more number of pieces1,3. The bone fracture healing time for a comminuted fracture is more. Comminuted fractures can occur from high-impact trauma like car accidents or heavy falls1.
First aid for the fracture:

This type of fracture is a small crack in the bone that develops due to repeated stress on the bone over time, which may weaken the bone and reduce its ability to withstand force. Hairline fractures commonly occur in the foot or lower leg due to repeated activities such as jogging or running1,3,6.
First aid for the fracture:

This type of fracture causes injury to the surrounding structures, such as muscles, nerves, blood vessels, arteries, and even the lining of the bone (periosteum). Can result from accidents, crushing injuries, or falls3.
First aid for the fracture:

In this type of fracture, a small piece of bone is pulled away from the main bone by a tendon or ligament attached to it. It usually occurs due to a sudden strong pull, such as during sports activities or from repeated stress over time. In rare cases, it can also happen after surgery or due to diseases that weaken the bone7.
First aid for the fracture:
This type of fracture results from pressing of the bones against each other3, where the bone may collapse. Compression fractures usually occur in the spine and may be caused by weakening of the bones due to osteoporosis or cancer3,8.
First aid for the fracture:
Note: The first aid tips provided are only for initial management and should never replace proper treatment. It is recommended to take the patient to the hospital as early as possible following an injury.
The most common approaches to diagnosing a bone fracture include:
Bone fracture treatment can be performed using either non-surgical or surgical methods, depending on the severity and type of injury.
Non-surgical treatment approaches include:
Surgical approaches for fracture are needed when nonsurgical options are not suitable and include:
Note: Treatment approaches are selected based on the types of bone fractures. Non-surgical methods should only be followed under the guidance of a doctor.
If surgical options are required, they should be performed by a qualified specialist. After surgery, adequate rest and proper care are important, and the patient should follow the doctor’s instructions to support safe and timely recovery.
The healing time for a bone fracture varies depending on the type and severity of the injury. While some fractures (e.g., fractures in the fingers) take 3 to 4 weeks to heal, others may need 6 to 8 weeks, 3 to 6 months, or even longer1. In children, the healing may be faster, while it might take more time in adults14 . More complex fractures, such as comminuted or complicated fractures, may require several months for complete recovery, especially if surgery is involved.
Several factors can affect the recovery process. These include the patient’s age, the type and location of the fracture, overall health, and the treatment method used1,3. Good nutrition (especially calcium and vitamin D supplementation), proper rest, and regular medical follow-up also play an important role in the healing process1,15.
Physiotherapy is an essential part of treatment and recovery after a fracture. Once the bones start healing, physiotherapy under expert guidance might help restore muscle strength, flexibility, and range of motion of the affected area4. It might help reduce stiffness and muscle weakness caused by extended periods of immobilisation. Normal activities can be resumed gradually, once the bones have healed and attained strength; however, it is important to follow medical guidance to avoid re-injury.
Also Read: How High Heels Affect the Body?
Here are some ways to help reduce the occurrence of bone fractures.
Also Read: Joint Pain During the Monsoon: Causes, Symptoms, Exercises & Relief Tips
The following signs and symptoms indicate the patient requires immediate medical attention:
Also Read: Sprained Ankle: What Is It, Causes, Symptoms & More
Bone fractures are common injuries that might vary in severity, but require timely medical attention for proper healing. Early diagnosis, an appropriate medical approach, and guided rehabilitation play an important role in recovery. By maintaining bone health and taking protective measures, the risk of fractures can be reduced, supporting overall mobility and quality of life.
Bone fractures can occur from trauma from accidents or sports injuries, due to low bone density (osteoporosis), repetitive usage of particular bones, such as from jogging or running1.
The initial approaches that can be employed following a fracture are managing bleeding, immobilising the injured area using a splint, and restricting the patient from moving3.
After a bone fracture, avoid moving the injured area or trying to straighten it, lifting or driving, and getting your cast wet3.
For a faster recovery from fracture, getting proper rest, taking a nutrient-rich diet, avoiding smoking and alcohol consumption, and having regular check-ups and follow-ups can help1,3.
The signs of a healing fracture may include a slow reduction in pain, reduced swelling and fading of bruises.
1. Fractures (Broken Bones). doi: https://orthoinfo.aaos.org/en/diseases–conditions/fractures-broken-bones/
2. Broken Bone. 2024. doi: https://medlineplus.gov/ency/article/000001.htm
3. Bone Fractures. 2022. doi: https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/bone-fractures
4. Open Fractures. doi: https://orthoinfo.aaos.org/en/diseases–conditions/open-fractures/
5. Atanelov Z, Bentley TP. Greenstick Fracture. 2023. doi: https://www.ncbi.nlm.nih.gov/books/NBK513279/
6. Fractures. 2024. doi: https://www.healthdirect.gov.au/fractures
7. McCoy JS, Nelson R. Avulsion Fractures. In: StatPearls. StatPearls Publishing; 2026. Accessed March 17, 2026. http://www.ncbi.nlm.nih.gov/books/NBK559168/
8. Compression Fracture. doi:https://www.cancer.gov/publications/dictionaries/cancer-terms/def/compression-fracture
9. Diagnosis of Fracture. doi:https://www.ncbi.nlm.nih.gov/books/NBK174863/
10. Sadineni RT. Imaging Patterns in MRI in Recent Bone Injuries Following Negative or Inconclusive Plain Radiographs. JCDR. Published online 2015. doi:10.7860/JCDR/2015/15451.6685 Available from: https://europepmc.org/article/pmc/4625309
11. Computer Tomography. 2025. doi: https://www.nibib.nih.gov/science-education/science-topics/computed-tomography-ct
12. Bone Graft. doi: https://medlineplus.gov/bonegrafts.html
13. Seidlitz C, Kip M. Chapter 1: Introduction to the Indications and Procedures. doi: https://www.ncbi.nlm.nih.gov/books/NBK546138/
14. Lindaman LM. Bone healing in children. Clin Podiatr Med Surg. 2001;18(1):97-108. doi: https://pubmed.ncbi.nlm.nih.gov/11344982/
15. Institute of Orthopaedic Research and Biomechanics, University of Ulm, Helmholtzstraße 14, 89081 Ulm, Germany, Fischer V, Haffner-Luntzer M, Amling M, Ignatius A. Calcium and vitamin D in bone fracture healing and post-traumatic bone turnover. eCM. 2018;35:365-385. doi:10.22203/eCM.v035a25. Available from: https://pubmed.ncbi.nlm.nih.gov/29931664/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
For couples, the journey to parenthood begins with hope and excitement. But sometimes when months pass without a positive pregnancy test, that hope slowly turns into worry, confusion, and even frustration. If this is how you feel, you’re not alone. Difficulty conceiving (for both men and women) is more common than most people realise.
Female infertility refers to the inability to get pregnant despite trying regularly. It could result from a variety of factors, ranging from hormonal imbalances to structural problems or underlying medical conditions. The reassuring part is that infertility is often manageable with early evaluation and timely intervention with the right medical support1,2.
In this blog, we will walk you through everything you need to know about female infertility, from common female infertility causes to available management options and when to seek medical help, allowing you to make well-informed choices about your reproductive health.
To better understand female infertility, let’s first understand how a pregnancy occurs. Each month, a woman’s ovaries release an egg (ovulation), which travels through the fallopian tube, where it may be fertilised by sperm. The fertilised egg then moves to the uterus, where it may implant and grow into a pregnancy3. For a pregnancy to occur, all these steps need to work together smoothly. A problem at any stage may make it more difficult to conceive (get pregnant).
Doctors usually define female infertility as not being able to conceive after one year of unprotected intercourse (or after 6 months for women above 35 years of age). Repeated miscarriages can also be considered a form of infertility1.
Infertility may be more common than many people think. Around 85% of couples conceive within a year, and the chances of getting pregnant each month are typically 15–20%. However, about 15% of couples worldwide face infertility, with female factors contributing to nearly half of these cases2.
Types of infertility in females are generally based on whether a woman has been pregnant before4:
Female infertility can occur when any step in the reproductive process is disrupted. This may happen if the ovaries do not produce healthy eggs, if the egg cannot travel from the ovaries to the uterus, or if a fertilised egg fails to implant properly in the uterine lining. In some cases, even after implantation, the embryo may not survive or develop normally5.The most common reasons for female infertility include:
The reproductive process is controlled by hormones regulated by the hypothalamus and pituitary glands (glands that are located in the brain and control many body functions). Any imbalance in this system can disrupt ovulation (release of a mature egg from the ovary). Conditions such as pituitary tumours or hypopituitarism (inadequate hormone production by the pituitary gland) can interfere with normal hormone levels and fertility3.
Problems with the ovaries can affect egg production or release. These may include2,4:
Damage or blockage in the fallopian tubes can prevent the egg and sperm from meeting. This is often caused by untreated sexually transmitted infections (STIs), complications from unsafe abortions, postpartum infections, or previous abdominal or pelvic surgeries3. Additionally, tubal damage may also occur due to genital tuberculosis (TB), which can cause scarring and blockage of the fallopian tubes6.
Conditions affecting the uterus can interfere with implantation of the fertilised egg or pregnancy. These may include3:
Note: In some cases, no clear cause may be identified. This is known as unexplained infertility2.
In many cases, infertility may not have any obvious symptoms. The only sign is difficulty in getting pregnant despite regular, unprotected intercourse. However, certain female infertility symptoms or signs can point toward underlying issues affecting fertility. Common signs and symptoms of female infertility include:
Certain factors can increase a woman’s risk of infertility by affecting ovulation, egg quality, or overall reproductive health. These risk factors may not directly cause infertility but can significantly reduce the chances of conception. Common risk factors include:
Diagnosis of infertility in females usually involves a combination of blood tests, imaging studies, and ovulation assessments to identify the underlying cause. These tests help evaluate hormone levels, ovarian function, and the structure of reproductive organs. Common diagnostic tests include:
A range of blood tests is used to evaluate hormonal balance and detect underlying conditions5,12,13:
Note: Your doctor may also suggest blood test packages that include parameters to check female reproductive health.
Also Read: What Is Ovulation? Understanding The Ovulation Process and Symptoms
Female infertility treatment depends on the underlying cause, age, and overall health. In many cases, a combination of approaches is used to improve the chances of conception. All of these options will be based on your doctor’s advice2:
Changes in lifestyle, such as weight management and quitting smoking, alcohol use, or recreational drug use can help preserve fertility. According to a recent study, lifestyle changes, including a weight loss of about 5–10%, can restore ovulation in 50–60% of obese women with PCOS.
Medications are often the first-line options, especially for women with ovulation disorders. They help stimulate ovulation and correct hormonal imbalances. Antibiotics may also be prescribed if infections are present.
When medications alone are not effective, assisted reproductive techniques may be recommended. These include:
Note: IUI is usually tried first in selected cases, while IVF is recommended when other treatments fail or in more complex conditions. However, success rates for both depend on factors such as age and ovarian reserve.
Also Read: IVF (In Vitro Fertilization): What is It, Procedure, Steps, Side Effects & More
Surgery may be needed to correct structural abnormalities that interfere with fertility. Procedures such as hysteroscopy or laparoscopy can help treat conditions like fibroids, endometriosis, or uterine abnormalities. Tubal surgeries may also be performed to restore normal function in selected cases.
Advanced options like the use of donor eggs or genetic testing of embryos can be considered in specific cases, especially when ovarian reserve is low or with increasing age.
While not all female infertility causes can be prevented, adopting healthy habits can support reproductive health and improve the chances of conception. Some options include15:
Note: Egg freezing (oocyte cryopreservation) allows women to preserve their eggs for future use. It is useful for those who wish to delay pregnancy or are undergoing medical treatments that may affect fertility. However, success rates are generally better when eggs are frozen at a younger age16.
Knowing when to seek medical help is important for early diagnosis and better outcomes. You should consider seeing a doctor if1,2,5:
Also Read: HIV Cure: Is it possible? Know the Symptoms and Treatment Options
Female infertility is a complex but common condition that can arise from a variety of factors, including hormonal imbalances, structural issues, lifestyle influences, and underlying medical conditions. While it can feel overwhelming, understanding female infertility causes, symptoms, and available diagnostic options is the first step toward effective management.
The encouraging part is that many cases of infertility are manageable, with a range of options (from medications and lifestyle modifications to advanced techniques like IVF) that could help improve fertility. Early evaluation, timely intervention, and a personalised approach to care can make a significant difference in infertility treatment.
Ovulation is just one part of conception. Pregnancy may still not happen due to issues like blocked fallopian tubes, poor egg quality, sperm-related factors, or problems with implantation2,5.
Ashwagandha may help reduce stress, but there is no strong evidence for its role in improving female fertility17. Therefore, it should never replace medical treatment.
Many causes are treatable or manageable, depending on the underlying issue2,4. Your doctor will help you with the right treatment based on your medical history.
In some cases, yes. Certain genetic and chromosomal conditions (such as Turner syndrome, fragile X premutation, and structural chromosomal abnormalities) may affect ovarian function and fertility2. However, not all infertility is genetic, and many causes may be unrelated to inherited factors.
There is no strong evidence that normal cell phone use causes female infertility18. However, limiting excessive exposure to radiation may still be considered a good precaution.
Typhoid itself usually does not cause infertility. However, severe or untreated infections may rarely lead to complications that could affect overall health19.
Stress alone may not directly cause infertility, but it can affect hormones and ovulation, making it harder to conceive15. So, managing stress may help improve overall fertility.
1. Female Infertility. Accessed April 29, 2026. https://medlineplus.gov/femaleinfertility.html
2. Adebisi OY, Singh M, Tobler KJ. Female Infertility. In: StatPearls. StatPearls Publishing; 2026. Accessed April 29, 2026. http://www.ncbi.nlm.nih.gov/books/NBK556033/
3. The menstrual cycle. Accessed May 1, 2026. https://womenshealth.gov/pregnancy/menstrual-cycle
4. Infertility. Accessed April 29, 2026. https://www.who.int/news-room/fact-sheets/detail/infertility
5. Infertility: MedlinePlus Medical Encyclopedia. Accessed April 29, 2026. https://medlineplus.gov/ency/article/001191.htm
6. Genital tuberculosis in females – PMC. Accessed April 30, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC5663156/
7. Attia GM, Alharbi OA, Aljohani RM. The Impact of Irregular Menstruation on Health: A Review of the Literature. Cureus. 15(11):e49146. doi:10.7759/cureus.49146 https://pmc.ncbi.nlm.nih.gov/articles/PMC10733621/
8. Harada T. Dysmenorrhea and Endometriosis in Young Women. Yonago Acta Med. 2013;56(4):81-84. https://pubmed.ncbi.nlm.nih.gov/24574576/
9. Uimari O, Subramaniam KS, Vollenhoven B, Tapmeier TT. Uterine Fibroids (Leiomyomata) and Heavy Menstrual Bleeding. Front Reprod Health. 2022;4:818243. doi:10.3389/frph.2022.818243 https://pubmed.ncbi.nlm.nih.gov/36303616/
10. Witchel SF, Oberfield SE, Peña AS. Polycystic Ovary Syndrome: Pathophysiology, Presentation, and Treatment With Emphasis on Adolescent Girls. J Endocr Soc. 2019;3(8):1545-1573. doi:10.1210/js.2019-00078 https://pubmed.ncbi.nlm.nih.gov/31384717/
11. Jain M, Carlson K, Singh M. Environmental Toxins and Infertility. In: StatPearls. StatPearls Publishing; 2026. Accessed April 29, 2026. http://www.ncbi.nlm.nih.gov/books/NBK576379/
12. Seckin B, Turkcapar F, Ozaksit G. Elevated day 3 FSH/LH ratio: a marker to predict IVF outcome in young and older women. J Assist Reprod Genet. 2012;29(3):231-236. doi:10.1007/s10815-011-9695-5 https://pubmed.ncbi.nlm.nih.gov/22183503/
13. Hendriks DJ, Mol BWJ, Bancsi LFJMM, Velde ER te, Broekmans FJM. The clomiphene citrate challenge test for the prediction of poor ovarian response and nonpregnancy in patients undergoing in vitro fertilization: a systematic review. Fertil Steril. 2006;86(4):807-818. doi:10.1016/j.fertnstert.2006.03.033 https://pubmed.ncbi.nlm.nih.gov/16962116/
14. Arvis P, Rongières C, Pirrello O, Lehert P. Reliability of AMH and AFC measurements and their correlation: a large multicenter study. J Assist Reprod Genet. 2022;39(5):1045-1053. doi:10.1007/s10815-022-02449-5 https://pubmed.ncbi.nlm.nih.gov/35243569/
15. Sharma R, Biedenharn KR, Fedor JM, Agarwal A. Lifestyle factors and reproductive health: taking control of your fertility. Reprod Biol Endocrinol RBE. 2013;11:66. doi:10.1186/1477-7827-11-66 https://pmc.ncbi.nlm.nih.gov/articles/PMC10135990/
16. Petropanagos A. Reproductive ‘Choice’ and Egg Freezing. Cancer Treat Res. 2010;156:223-235. doi:10.1007/978-1-4419-6518-9_17 https://pmc.ncbi.nlm.nih.gov/articles/PMC3086489/
17. Vani I, Muralidhar G, Rao BS. A prospective, randomized, double-blind, placebo-controlled study on efficacy and safety of Ashwagandha root extract (Withania somnifera) for managing menopausal symptoms in women. Front Reprod Health. 7:1647721. doi:10.3389/frph.2025.1647721 https://pubmed.ncbi.nlm.nih.gov/41561822/
18. Merhi ZO. Challenging cell phone impact on reproduction: A Review. J Assist Reprod Genet. 2012;29(4):293-297. doi:10.1007/s10815-012-9722-1 https://pmc.ncbi.nlm.nih.gov/articles/PMC3309987/
19. Marchello CS, Birkhold M, Crump JA. Complications and mortality of typhoid fever: A global systematic review and meta-analysis. J Infect. 2020;81(6):902-910. doi:10.1016/j.jinf.2020.10.030 https://pubmed.ncbi.nlm.nih.gov/33144193/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Breast sagging is a condition where the breast skin and tissues slowly stretch, causing the breasts to move downward over time1. It can be seen in different age groups and breast sizes, but becomes more noticeable in women in their late 20s to 30s and beyond. Studies show it is more noticeable with increasing age and after childbirth due to pregnancy-related body changes1,2. It may also occur due to weight changes and loss of skin elasticity1. This blog will explain the causes of sagging breasts and its treatment options, home remedies, and prevention tips.
Sagging breasts, meaning breast ptosis in medical terms, is a condition where the breast slowly moves lower on the chest and loses its natural lifted shape. In a healthy youthful breast, the nipple sits near the most outward point of the breast, and the lower part looks full and rounded. When this balance changes, the breast may look longer, flatter, or droopier. There are different patterns in which breast sagging can appear:
Several changes inside the body can lead to sagging breasts. The supporting tissues in the breast gradually stretch over time, especially with changes like pregnancy, weight fluctuations, and ageing that affect how the breast maintains its shape. As the skin also loses firmness and elasticity, it becomes less able to hold the breast in an elevated position. Together, these changes slowly alter breast shape and position, leading to a lowering of the breast and less firm appearance over time3.
Did You Know?

Breast sagging is assessed by checking how low the nipple sits compared to the inframammary fold (the fold under the breast)4. The Regnault classification system is used to describe how much the breast has sagged6.
These are the 3 main grades of breast sagging4,6:
Sometimes, the nipple stays near the fold, but most of the breast tissue hangs lower, this is called pseudoptosis6. Doctors use these grades to understand how much the breasts have sagged and to decide the right treatment or surgery if needed. Next, let us look at the causes of sagging breasts.
Breast sagging occurs when the skin, inner support, and breast tissue change over time. Below are some breast sagging reasons4,5:

In some people, the skin may be less elastic, and the supportive bands (Cooper’s ligaments) within the breast may be weaker. When these support bands become loose, the breast may start to sag.

Breast heaviness and density can affect how the breast holds its shape as they place strain on the supporting tissues, which may contribute to sagging over time.

These may also contribute to breast sagging. Skin elasticity, collagen quality, and connective tissue strength differ from person to person. Because of these inherited traits, the skin and supportive bands in the breasts may stretch more easily over time in some individuals causing breast sagging7.

During pregnancy, the skin and inner support bands can lose their strength. Weight loss can also change the breast and lead to sagging. Weight cycling (yo-yo dieting) is a potential risk factor for breast sagging. Repeated instances of weight loss and weight gain can stretch and loosen breast skin multiple times, reducing its elasticity and weakening connective tissue support. Over time, this may contribute to breast ptosis, especially after major or repeated weight fluctuations8,9.

As women grow older, the skin and soft tissue support inside the breast become weaker, leading to sagging18.

Hormone changes after pregnancy or menopause can gradually affect breast volume and skin and tissue support over time, which may contribute to a less firm appearance. After menopause, a drop in oestrogen may cause the loss of breast fat, glandular tissue, and supporting structures, which makes the breasts more prone to sagging. The connective tissue also becomes less elastic, and the areola may shrink, while the nipple may slightly turn inward over time10.

Smoking and too much sun exposure can damage the breast tissues.
These causes can act together and slowly change the shape of the breast over time. In the next section, we will look at different ways to manage breast sagging.
The use of non-surgical and surgical options for breast sagging treatment depends on how mild or severe the condition is.
Non-surgical care mainly focuses on improving support and appearance through supportive bras, exercise, and skin care.
Surgical treatment is an option when correction may be needed in the position, shape, or volume of the breasts. Surgery can lift sagging breasts significantly, as it can remove the extra skin, reshape the breast tissue, and improve breast position.
The procedure is selected based on the degree of sagging and whether volume correction is also needed4. This allows the treatment to be tailored to individual breast shape and structure for a more balanced result.
Breast sagging is a natural change that can happen over time due to different internal and external factors. While it cannot be fully avoided, these simple steps may help support breast tissue health.

Smoking can reduce the normal elasticity of the skin, including elasticity of the skin around the breasts. Avoiding smoking helps maintain healthier and more supportive skin over time5.

Too much sun exposure can damage the skin fibres and reduce skin tightness. This may slowly affect breast tissues4. Using sunscreen regularly helps protect the skin from UV rays. SPF 30 or higher is recommended23.

Breast sagging may be seen more in people who have higher body weight and higher BMI5. Keeping a healthy weight by eating balanced food, doing regular exercise, sleeping well, and managing stress may help support overall body and breast health24.

Women who rarely use bras may have less support for the soft tissues of the breasts, which can increase strain over time. Using a properly fitted bra can help provide better support and reduce stress on breast tissues during daily activities5,11.

Frequent high-impact exercises can cause movement-related discomfort and put stress on the soft tissues of the breasts if proper breast support is not used5. High-impact exercise means activities like running or jumping, where both feet leave the ground and the body feels repeated impact25. So, it is advisable to include a variety of exercises in your routine and allow enough rest between sessions26.
These simple habits may help support skin health and reduce the factors associated with breast sagging over time.
1. Myth: Breast sagging happens only because of pregnancy.
Fact: No. Breast sagging can also happen when the skin becomes weak, the support tissues inside the breast become less strong, or when body weight changes over time. Ageing can also lead to breast sagging4.
2. Myth: Only old age causes breast sagging.
Fact: No. Breast skin can also be affected by smoking (weakens the skin), too much sun exposure (damages the skin), and changes in the body during pregnancy or menopause4.
3. Myth: Breastfeeding always causes breast sagging.
Fact: No. Studies show that breastfeeding and the number of pregnancies do not always directly cause breast sagging. Breast shape changes depend more on skin strength, strength of the supportive ligaments in the breasts, ageing, and other body changes5.
You should consult a doctor if you notice signs of breast ptosis (sagging) along with changes that may be concerning or different from usual age-related sagging.
These may include cosmetic changes (changes related to the appearance) due to ageing18, pregnancy, or weight fluctuations, such as:
You should also seek medical attention if you notice any of the following red flag symptoms that may need evaluation:
A doctor will examine your breast, check for underlying causes, and guide you on whether any treatment or follow-up is needed.
Breast sagging is a gradual change that happens over time due to ageing, pregnancy, weight changes, and hormonal factors that affect the skin and tissues supporting the breasts. While non-surgical methods like supportive bras, exercise, and skin care may help improve comfort and appearance, they cannot reverse the condition. Surgical options such as breast lift or augmentation are the only methods that can significantly correct breast shape and position when needed.
Also Read: Can You Increase Your Breast Size Naturally? Here’s What Doctors Want You To Know
Sagging breasts usually do not become fully firm again on their own because the skin and supportive tissues become loose over time. However, doctors can help improve breast shape and firmness using treatments like mastopexy (breast lift surgery), depending on the severity of the sagging4.
Breast ptosis can occur at any age and in any breast size, but it is mainly associated with ageing, pregnancy, weight changes, and hormonal factors1. It is more common after late 20s, and its occurrence generally increases in the 30s and 40s due to these progressive changes2.
No specific vitamin deficiency directly causes sagging breasts. However, vitamins A, C, and E support skin elasticity and collagen formation, so their deficiency may have a small effect on skin firmness28. Breast ptosis is mainly linked to ageing, pregnancy, weight changes, and hormonal factors rather than vitamins alone1.
Wearing a bra all the time may give support and comfort, but it does not stop breasts from sagging. Sagging occurs because of causes such as ageing, pregnancy, and gravity. A bra only helps with support and comfort rather than preventing these natural changes11.
Hormones are not the direct cause of breast sagging. Sagging is mainly caused by changes in breast tissue, volume, and skin support, leading to gradual loss of firmness over time due to the effect of hormones like oestrogen, progesterone, and prolactin during pregnancy and menopause11,29,30.
Exercise may help improve the appearance of sagging breasts. Strength training exercises like push-ups, chest presses, and chest flys strengthen the pectoral muscles underneath the breasts. This does not change breast tissue itself, but it improves the posture22 and gives a firmer, more lifted appearance14.
1. Martinez AA, Chung S. Breast Ptosis. In: StatPearls [Internet]. StatPearls Publishing; 2023. Accessed April 24, 2026. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK567792/
2. Kim SJ, Kim M, Kim MJ. The Affecting Factors of Breast Anthropometry in Korean Women. Breastfeed Med. 2014;9(2):73-78. doi:10.1089/bfm.2013.0068. Available from: https://pubmed.ncbi.nlm.nih.gov/24180472/
3. Hammond DC. Mastopexy. In: Atlas of Aesthetic Breast Surgery. Elsevier; 2009:83-128. doi:10.1016/B978-1-4160-3184-0.00005-4. Available from: https://www.researchgate.net/publication/281874844_Atlas_of_Aesthetic_Breast_Surgery
4. Harrak SE, Jaadi D, Sqalli H, et al. Mastopexy: Management of Breast Ptosis and Complications. SAS J Surg. 2021;7(10):590-595. doi:10.36347/sasjs.2021.v07i10.015. Available from: https://saspublishers.com/media/articles/SASJS_710_590-595.pdf
5. (PDF) A Study on Predisposing Factors to Breast Ptosis. ResearchGate. Accessed April 24, 2026. Available from: https://www.researchgate.net/publication/325793381_A_Study_on_Predisposing_Factors_to_Breast_Ptosis
6. Breast Ptosis – Abstract – Europe PMC. Accessed April 24, 2026. Available from: https://europepmc.org/article/nbk/nbk567792#_article-73063_s1_
7. Geusens B, Haykal D. Genetic profiling and precision skin care: a review. Front Genet. 2025;16:1559510. doi:10.3389/fgene.2025.1559510. Available from: https://pubmed.ncbi.nlm.nih.gov/40529811/
8. Colicchia G, Di Pietro V, Cervelli V. Mastoplasty after massive weight loss: Redefinition and stabilization of the breast mound with submuscular autoprosthesis. J Cutan Aesthetic Surg. 2019;12(3):164. doi:10.4103/JCAS.JCAS_48_18. Available from: https://pubmed.ncbi.nlm.nih.gov/31619888/
9. Thillainadesan S, Lambert A, Cooke KC, et al. The metabolic consequences of ‘yo-yo’ dieting are markedly influenced by genetic diversity. Int J Obes. 2024;48(8):1170-1179. doi:10.1038/s41366-024-01542-2. Available from: https://pubmed.ncbi.nlm.nih.gov/38961153/
10. Aging changes in the breast: MedlinePlus Medical Encyclopedia. Accessed April 27, 2026. Available from: https://medlineplus.gov/ency/article/003999.htm
11. Isono M, Tateoka Y. Fundamental Research on the Invention of Breast Support Underwear with a Focus on Women’s Comfort. Sensors. 2022;23(1):25. doi:10.3390/s23010025. Available from: https://www.mdpi.com/1424-8220/23/1/25
12. McGhee DE, Steele JR, Zealey WJ, Takacs GJ. Bra–breast forces generated in women with large breasts while standing and during treadmill running: Implications for sports bra design. Appl Ergon. 2013;44(1):112-118. doi:10.1016/j.apergo.2012.05.006. Available from: https://pubmed.ncbi.nlm.nih.gov/22742876/
13. Rivard AB, Peterson DC. Anatomy, Thorax, Breast. In: StatPearls [Internet]. StatPearls Publishing; 2023. Accessed April 24, 2026. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519575/
14. Schütz P, Zimmer P, Zeidler F, et al. Chest Exercises: Movement and Loading of Shoulder, Elbow and Wrist Joints. Sports. 2022;10(2):19. doi:10.3390/sports10020019. Available from: https://pubmed.ncbi.nlm.nih.gov/35202059/
15. Ibrahim AM, Sinno HH, Izadpanah A, Vorstenbosch J. Mastopexy for breast ptosis: Utility outcomes of population preferences. Plast Surg. 2015;23(2). doi:10.4172/plastic-surgery.1000916. Available from: https://pubmed.ncbi.nlm.nih.gov/26090352/
16. Ganceviciene R, Liakou AI, Theodoridis A, Makrantonaki E, Zouboulis CC. Skin anti-aging strategies. Dermatoendocrinol. 2012;4(3):308-319. doi:10.4161/derm.22804. Available from: https://pubmed.ncbi.nlm.nih.gov/23467476/
17. He X, Wan F, Su W, Xie W. Research Progress on Skin Aging and Active Ingredients. Molecules. 2023;28(14):5556. doi:10.3390/molecules28145556. Available from: https://pubmed.ncbi.nlm.nih.gov/37513428/
18. Fernandes A, Rodrigues PM, Pintado M, Tavaria FK. A systematic review of natural products for skin applications: Targeting inflammation, wound healing, and photo-ageing. Phytomedicine. 2023;115:154824. doi:10.1016/j.phymed.2023.154824. Available from: https://pubmed.ncbi.nlm.nih.gov/37119762/
19. Nagrik SU, Shivshankar M., Chharre VS, Dhage SM, Borey VS. Role of aloe vera in skincare: exploring its therapeutic benefits, formulations, and future innovations. Yemen J Med. 2024;03(03):197-206. doi:10.63475/j.yjom.2024.021. Available from: https://www.researchgate.net/publication/387072320_Role_of_aloe_vera_in_skincare_exploring_its_therapeutic_benefits_formulations_and_future_innovations
20. Prakoeswa CRS, Damayanti, Anggraeni S, et al. The Role of Moisturizer Containing Anti‐inflammatory on Skin Hydration in Mild‐Moderate Atopic Dermatitis Patients. Guglielmo A, ed. Dermatol Res Pract. 2024;2024(1):3586393. doi:10.1155/drp/3586393. Available from: https://pubmed.ncbi.nlm.nih.gov/39741562/
21. Breast augmentation surgery: MedlinePlus Medical Encyclopedia. Accessed April 24, 2026. Available from: https://medlineplus.gov/ency/article/002984.htm
22. Dung R. Managing Kyphosis: Preventive Strategies and Therapeutic Approaches for Spinal Health. 12(12). Available from: https://www.omicsonline.org/open-access-pdfs/managing-kyphosis-preventive-strategies-and-therapeutic-approaches-for-spinal-health.pdf
23. Faizan P, Prabhas M, Sharma DT. SUNSCREEN AS A COSMETIC PRODUCT: A COMPREHENSIVE REVIEW. Available from: https://www.ijarp.com/myimgup/994079394IJARP-2351.pdf
24. Steps for Losing Weight | Healthy Weight and Growth | CDC. Accessed April 24, 2026. Available from: https://www.cdc.gov/healthy-weight-growth/losing-weight/index.html
25. Khowailed IA, Pinjuv-Turney J, Lu C, Lee H. Stress Incontinence during Different High-Impact Exercises in Women: A Pilot Survey. Int J Environ Res Public Health. 2020;17(22):8372. doi:10.3390/ijerph17228372. Available from: https://pubmed.ncbi.nlm.nih.gov/33198262/
26. 10 Tips for Exercising Safely. Harvard Health. May 4, 2010. Accessed April 24, 2026. Available from: https://www.health.harvard.edu/healthbeat/10-tips-for-exercising-safely
27. Signs and Symptoms of Breast Cancer – NCI. Accessed April 24, 2026. Available from: https://www.cancer.gov/types/breast/symptoms
28. Januszewski J, Forma A, Zembala J, et al. Nutritional Supplements for Skin Health—A Review of What Should Be Chosen and Why. Medicina (Mex). 2023;60(1):68. doi:10.3390/medicina60010068. Available from: https://pubmed.ncbi.nlm.nih.gov/38256329/
29. Mammary Tissue Changes During Pregnancy and Breastfeeding | Springer Nature Link. Accessed April 24, 2026. Available from: https://link.springer.com/chapter/10.1007/978-3-030-43840-1_14
30. Ahmed G. El-Din Osman, M.D. MKhA MD;, Ahmed Ramadan El Sabbagh, M.Sc. SAAF MD; Comparison between Augmentation Mastopexy in One Session and Two Separate Sessions. Med J Cairo Univ. 2020;88(12):1985-1999. doi:10.21608/mjcu.2020.125137. Available from: https://mail.medicaljournalofcairouniversity.net/index.php/2014-10-22-23-17-30/vol-88-december-2020/4767-comparison-between-augmentation-mastopexy-in-one-session-and-two-separate-sessions
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Cancer can be confusing, especially when people talk about genes. Some people think that if cancer runs in the family, they will definitely get it. Others believe cancer happens randomly and has nothing to do with genes. The truth lies somewhere in the middle.
Most cancers develop from gene changes that happen during the lifetime of an individual due to factors such as aging, lifestyle, and environment, though some cancers can be inherited from parents1,2. However, cancer itself doesn’t pass from parents to children, and the changes in cancer cells also aren’t passed down. But for certain cancers, parents can pass on some genes that increase the chance of developing that cancer in the offspring (subsequent generation)1. Understanding this helps people know their risk better and take appropriate measures.
In this blog, we will explore whether cancer is a genetic disease or not, explain the difference between somatic and hereditary cancers, and discuss how family history and genetic testing can help identify individuals at a higher risk.
Cancer is a genetic disease, but it is not always inherited. Cancer develops when specific genes undergo mutations (changes) that affect how cells grow, divide, and repair themselves. These mutations can cause cells to proliferate uncontrollably, resulting in cancer cell formation. These genetic changes are the root cause of all cancers1.
Genetic changes can happen in two different ways:
This is the most common type. Here, gene changes occur during a person’s lifetime. They are not present at birth and are not handed down to the generations. These genetic changes or mutations may be caused by aging, environmental exposures (such as pollution and radiation), lifestyle factors (such as smoking, poor diet, or lack of exercise), infections, etc1,2.
This type is less common (only up to 10% of cancer are caused by inherited gene changes)1. Here a person acquires a gene mutation from their parents. This mutation is present in their cells from early life and can increase the risk of certain cancers. These inherited changes can also be passed on to the next generation from father’s sperm or mother’s egg (germ cells). Examples of hereditary cancer syndromes include BRCA1/BRCA2-related breast and ovarian cancer and Lynch syndrome (an inherited condition that increases a person’s risk of developing certain cancers, especially colon and endometrial cancer, at an early age)3.
So, genetic mutations are responsible for the occurrence of all cancers, but only a small percentage of cancers occur due to certain genes being passed down from parents during conception.
Cancer can develop due to different types of changes in our genes. These changes affect how cells grow and behave. Here are the main types:
The following are some signs which say you may have a hereditary cancer:
Note: These signs don’t guarantee that cancer is hereditary, but they may indicate a higher risk and the need for medical advice or genetic testing.
Genetic testing in cancer is usually done to detect the presence of inherited gene mutations that increase the risk of developing certain type of cancers (presence of germline mutations). Sometimes, if a person is already diagnosed with cancer, genetic testing may be done to check for the gene mutations associated with the cancer (tumour or somatic genetic testing). There are numerous types of genetic tests available now, and many more are still being developed8.
For predicting cancer risk, genetic testing checks for the presence of specific genes that may raise a person’s chance of getting a cancer. It mainly helps to:
In somatic (tumour) genetic testing, the DNA of cancer cells is checked to find changes that led to the tumour. These tests do not detect inherited cancer risk but help doctors in the following way:
Genetic cancer testing checks your DNA to find inherited changes that may increase your risk of certain cancers. It is performed through the following steps:
Note: Testing is usually recommended based on trusted medical guidelines.
If you observe any warning symptoms or have a family history that puts you at risk for cancer, you should contact a doctor. Early medical guidance can aid in immediate detection and better results.
Signs and Symptoms That Need Medical Attention
The following are some warning signs that you should not ignore and seek immediate medical attention for:
Family History and Risk-Related Situations
Family history might enhance your cancer risk and should not be ignored, especially if you are experiencing symptoms. Multiple family members with cancer, cancer at a younger age, the same type of disease returning in the family, having a close relative with cancer, or a family history of related cancers such as breast and ovarian cancer are all warning signals that should be discussed with a doctor9.
Along with consulting a doctor, opting for a comprehensive full-body checkup can help in early detection of potential health risks.
Cancer is a genetic disease however not all cancers are passed on. Understanding the difference between somatic and hereditary cancer might help you determine your risk and take appropriate action. Paying attention to family history and considering genetic testing as needed can help with early detection and treatment. Taking informed action now can result in improved health outcomes tomorrow.
Also Read: Types of Cancer: Symptoms, Early Signs, Diagnosis & More
Inherited gene changes can’t be changed, but cancer can often be prevented or found early through regular screening and healthy lifestyle choices3.
Many cancers are treatable if detected early, while some are more difficult to treat, particularly in advanced stages. Cancers such as pancreatic cancer, are often diagnosed at advanced stages and have poor survival rates, making them more difficult to treat. Similarly, oesophageal cancer, if not detected at an early stage, can spread to the other parts, making recovery difficult11.
The most common cancers which can be inherited are breast cancer, ovarian cancer, uterine cancer, prostate cancer, pancreatic and colorectal cancer1,8.
No, cancer is not 100% hereditary. Only a small percentage (10%) of cancers are inherited, while most develop due to gene changes that occur during a person’s lifetime1.
Yes, cancer occurrence may skip a generation. However, the faulty gene is still passed down, but not everyone who has it will develop cancer1.
An abnormal gene that increases cancer risk can come from either the mother or the father. Only about 5-10% of cancers are inherited; that is they are passed down through genes in sperm or egg cells1.
Cancer is usually not directly inherited, but some gene changes passed from parents (through sperm or egg) can increase cancer risk. These are found in all cells of the body and are linked to about 5-10% of cancers1.
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Many women experience issues like irregular periods, sudden weight gain, acne, or mood swings but may not immediately understand the cause. These can often be linked to polycystic ovarian disease (PCOD), or polycystic ovarian syndrome (PCOS), conditions which are associated with hormonal imbalances, mainly affecting the ovaries, but can also affect other parts of the body1.
PCOD and PCOS are often used interchangeably, but they are slightly different. PCOD is usually identified through ultrasound scans, while PCOS is a more serious condition diagnosed based on symptoms and involves greater hormonal and metabolic imbalances.
Today, a large number of women are affected by PCOD, especially due to changes in lifestyle, stress, and eating habits2. Diet and lifestyle can play an important role in managing the condition, and making healthier food choices may help improve symptoms and support overall health.
This blog about PCOD diet chart will help you understand what foods to eat and what to avoid if you have PCOD. We will also provide you with some sample meal plans and simple lifestyle tips that can help you manage PCOD effectively.
PCOD is the presence of polycystic changes in the ovaries, commonly seen in women of reproductive age. They arise when the follicles (small sacs in the ovary that release egg) do not grow properly. Instead of developing and releasing an egg during ovulation, these follicles remain tiny and form fluid-filled sacs, giving the polycystic appearance on ultrasound scans1,3.
A polycystic ovary is usually diagnosed when:
These changes are mainly due to a hormone imbalance, which prevents the follicles from maturing and releasing an egg. As ovulation may not happen regularly, the menstrual cycle gets disturbed, and in some cases, it can affect fertility1.
Not all women will have the same symptoms, but common ones include:
Diet plays a central role in managing PCOD because the condition is closely linked to how the body processes hormones, sugar, and fat. The right food choices can help balance hormones, control blood sugar, and reduce symptoms. The following says why diet is important to manage PCOD.
The following are a list of foods for PCOD management that you can consider:

Foods with low glycaemic index that is those that do not cause a spike in insulin after consumption like high-fibre foods7, help control blood sugar levels and improve hormonal balance6,8. These include:

They support muscle health and help in weight management, which is important to manage PCOD symptoms6,9. These include:

Foods rich in healthy fats such as omega-3 and MUFA are helpful in managing PCOD6. They help improve insulin sensitivity, reduce inflammation, and also support weight management10. These include:

Foods rich in micronutrients such as Vitamins D and other vitamins and minerals can help reduce inflammation, improve insulin sensitivity and enhance metabolic health, thereby supporting PCOD management6,11. These include:
Note: Certain foods may trigger allergic reactions in some individuals. Such foods should be avoided. Also, it is recommended to consult a doctor or dietitian before making any dietary changes if you have PCOD and other associated conditions like diabetes.
There are several foods to be avoided if you have PCOD, as they can negatively impact your health. The following are some foods to avoid in PCOD:

These digest very fast and contribute to sudden glucose spikes. They also cause insulin resistance which can worsen PCOD6,12. These include:

These contribute to rapid increase in blood sugar, leading to higher insulin production and eventually insulin resistance. This negatively affects metabolism and can aggravate PCOD symptoms6,12.

These foods are high in salt and unhealthy fats. They can cause weight gain and increase the risk of obesity, diabetes and other inflammatory diseases, in turn negatively affectively PCOD6,13.

These foods are high in unhealthy fats. They cause inflammation and contribute to obesity, diabetes, cardiovascular disease, etc., by worsening PCOD14.
The following table shows a 7-day diet plan which can be considered a PCOD diet chart for weight loss.
| Day | Breakfast | Mid-Morning Snack | Lunch | Evening Snack | Dinner |
| Day 1 | Spinach and banana smoothie with flaxseeds | 1 apple + handful of soaked almonds | Quinoa pulao with mixed vegetables + cucumber raita. | Tea + roasted chana | 2 chapatis + vegetable curry |
| Day 2 | Moong dal dosa (or besan chilla) with mint chutney | Coconut water + 1 Pear. | 2 multigrain rotis + rajma curry + spinach fry + cucumber salad | 1 cup Low-fat yogurt | Broken wheat khichdi or tofu stir-fry. |
| Day 3 | Vegetable omelette + whole wheat toast | Watermelon bowl | 1 cup brown rice + methi dal + stir-fried french beans | Roasted makhana (foxnuts) + green tea | Moong dal khichdi+ sauteed vegetables |
| Day 4 | Spinach and vegetable poha (made by adding peanuts & peas) + 1 glass of milk (low-fat) | A small bowl of mixed berries | ½ cup brown rice + 1 cup lentil curry + 1 cup ladies finger curry + salad | 1 boiled egg + a glass of low-fat milk | 2 Small multigrain rotis+ grilled chicken / paneer |
| Day 5 | Vegetable oats + 1 boiled egg | 1 Guava or pomegranate | 2 bajra rotis + Chana dal + cucumber-tomato salad | Buttermilk + roasted seeds | Vegetable-stuffed besan cheela (less oil) |
| Day 6 | Millet dosa with tomato chutney | Fruit salad with sunflower seeds | Mixed dal + quinoa rice + roasted veggies | 1 bowl Papaya slices | Vegetable soup + salad + paneer/tofu |
| Day 7 | Ragi (finger millet) porridge with nuts | 1 small orange + few pumpkin seeds | Brown rice + sambar + vegetable stir-fry | 2 small ragi laddus | 2 chapatis+ paneer tikka |
Note: This 7-day diet plan is for general guidance only. Everyone’s needs may differ based on age, health, and lifestyle. It is best to consult a doctor or dietitian to get a customised diet for PCOD patients.
Along with a proper diet, the following lifestyle tips might help you manage your PCOD symptoms.
Sticking to a proper diet is not always an easy task. Consistency is the key. The following are some tips that might help you stick to your PCOD diet.
Also Read: Simple Home Remedies to Help Ease PCOS Symptoms
A healthy lifestyle and a well-balanced diet are required for effective management of PCOD. Choosing the proper meals, being active, controlling stress, and practising healthy daily routines can all assist in improving hormonal balance and alleviating symptoms. Consistency is more important than perfection, so small, regular efforts can have a significant impact over time. With the right strategy and mindset, PCOD can be effectively managed, leading to improved overall health and well-being.
Yes, a PCOD patient can eat curd, as it is a probiotic. According to some studies, probiotics help in managing fasting blood sugar, reduce inflammation and improve insulin activity in women with PCOD6.
Losing 5 kg in a month can be difficult, but you can aim for it by eating healthy (less sugar and junk food, more fruits, vegetables, and protein). Regular exercise, good sleep, and managing stress can help your body work better and support weight management5,6,12,14.
PCOD can be managed through diet, but it should be combined with stress management, regular physical activity, proper sleep, and healthy lifestyle habits for better results. However, PCOD cannot be completely cured; it needs long-term management with these factors5
Yes, dates can be included in the diet for PCOD, as they are rich in fibre, natural energy, vitamins, and minerals. However, they should be consumed in moderation due to their high natural sugar content, which may affect blood glucose levels if taken in excess18.
Herbal infusion made from ingredients like cinnamon, aloe vera, green tea, etc., are said to reduce the symptoms of PCOD, as they are rich in several antioxidants and have anti-inflammatory properties. However, more research is needed to confirm the potential benefits of these herbal infusions for PCOD management5. The best drink therefore, you may choose is just plain water, which will help you stay hydrated and support your metabolism and overall health16.
1. Polycystic Ovary Syndrome. 2024. Available from: https://medlineplus.gov/polycysticovarysyndrome.html
2. Sharma A, Sarwal Y, Devi NK, Saraswathy KN. Polycystic Ovary Syndrome prevalence and associated sociodemographic risk factors: a study among young adults in Delhi NCR, India. Reprod Health. 2025;22(1):61. doi:10.1186/s12978-025-02019-9. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12039125/
3. Polycystic ovarian syndrome (PCOS). 2024. Available from: https://www.healthdirect.gov.au/polycystic-ovarian-syndrome-pcos#symptoms
4. Nallaparaju LS. QUANTIFYING THE PREVALENCE AND INTERDEPENDENT RELATIONSHIPOF PCOD, OBESITY, AND DEPRESSION – A PROSPECTIVE OBSERVATIONAL, POLYCENTRIC STUDY. World Journal of Pharmaceutical Research. 12(7):732-764. Available from: https://wjpr.s3.ap-south-1.amazonaws.com/article_issue/57fb03a2e4edae203d6b8262b656e58b.pdf
5. Szczuko M, Kikut J, Szczuko U, et al. Nutrition Strategy and Life Style in Polycystic Ovary Syndrome—Narrative Review. Nutrients. 2021;13(7):2452. doi:10.3390/nu13072452. Available from: https://pubmed.ncbi.nlm.nih.gov/34371961/
6. Muhammed Saeed AA, Noreen S, Awlqadr FH, et al. Nutritional and herbal interventions for polycystic ovary syndrome (PCOS): a comprehensive review of dietary approaches, macronutrient impact, and herbal medicine in management. J Health Popul Nutr. 2025;44(1):143. doi:10.1186/s41043-025-00899-y. Available from: https://pubmed.ncbi.nlm.nih.gov/40317096/
7. High-fiber foods. 2024. Available from: https://medlineplus.gov/ency/patientinstructions/000193.htm
8. Whole Grains. Available from: https://nutritionsource.hsph.harvard.edu/what-should-you-eat/whole-grains/
9. Protein. Available from: https://nutritionsource.hsph.harvard.edu/what-should-you-eat/protein/
10. DiNicolantonio JJ, O’Keefe JH. Good Fats versus Bad Fats: A Comparison of Fatty Acids in the Promotion of Insulin Resistance, Inflammation, and Obesity. Mo Med. 2017;114(4):303-307. Available from: https://pubmed.ncbi.nlm.nih.gov/30228616/
11. Yu X, Pu H, Voss M. Overview of anti-inflammatory diets and their promising effects on non-communicable diseases. Br J Nutr. 2024;132(7):898-918. doi:10.1017/S0007114524001405. Available from: https://pubmed.ncbi.nlm.nih.gov/39411832/
12. Maffetone P, Laursen PB. Refined carbohydrates and the overfat pandemic: implications for brain health and public health policy. Front Public Health. 2025;13:1585680. doi:10.3389/fpubh.2025.1585680. Available from: https://pubmed.ncbi.nlm.nih.gov/41229472/
13. Mititelu M, Oancea CN, Neacșu SM, et al. Evaluation of Junk Food Consumption and the Risk Related to Consumer Health among the Romanian Population. Nutrients. 2023;15(16):3591. doi:10.3390/nu15163591. Available from: https://pubmed.ncbi.nlm.nih.gov/37630781/
14. Gadiraju T, Patel Y, Gaziano J, Djoussé L. Fried Food Consumption and Cardiovascular Health: A Review of Current Evidence. Nutrients. 2015;7(10):8424-8430. doi:10.3390/nu7105404. Available from: https://pubmed.ncbi.nlm.nih.gov/26457715/
15. Salajegheh Z, Ahmadi A, Shahrahmani H, et al. Mindfulness-based stress reduction (MBSR) effects on the worries of women with poly cystic ovary syndrome (PCOS). BMC Psychiatry. 2023;23(1):185. doi:10.1186/s12888-023-04671-6. Available from: https://pubmed.ncbi.nlm.nih.gov/36944940/
16. Water – a vital nutrient. 2026. Available from: https://www.betterhealth.vic.gov.au/health/healthyliving/water-a-vital-nutrient
17. Polycystic ovary syndrome (PCOS). 2024. Available from: https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/polycystic-ovarian-syndrome-pcos
18. Awan KA, Yaqoob S, Ul‐Haq I, et al. Therapeutic Power of Date Fruit (Phoenix dactylifera L.): A Nutrient‐Rich Superfood for Holistic Health and Disease Prevention. Food Science & Nutrition. 2025;13(9):e70896. doi:10.1002/fsn3.70896. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12415069/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
1
For any big disease, early detection plays a crucial role in improving the chances of successful treatment and survival. One such disease is cancer, where abnormal body cells grow and multiply uncontrollably, and can invade and damage nearby healthy tissues1.
There are several types of cancer, and a lot of them develop gradually and may show only mild signs in the early stages2. These signs are often ignored or mistaken for other health conditions. Being aware of these early warning signs can help individuals seek medical advice at the right time and take appropriate action2.
In addition to recognising symptoms, regular screening programmes such as tumour marker tests, mammography, colonoscopy, and Pap smear also play a key role in the early detection of certain cancers2,3 often before symptoms appear.
In this article, we will discuss more early warning signs of cancer, why they are important and when to seek medical attention. The aim here is not to create fear, but to encourage awareness and regular health monitoring for early detection of diseases like cancer.
Warning signs of cancer are unusual or unexpected changes in the body which may indicate that something is not functioning normally1. These can be visible physical symptoms (lumps, bleeding, etc.) or internal symptoms (fatigue, digestive problems, etc.)1,4.
In many cases, early-stage cancer may not cause any noticeable symptoms for months or even years1. Symptoms often appear later, as the disease progresses and begins to affect surrounding tissues or body functions. However, it is important to remember that these symptoms are not always caused by cancer they may also result from common illnesses or temporary health issues.
Still, persistent, recurring, or worsening symptoms should not be ignored. In addition, certain symptoms, such as unexplained bleeding2, coughing up blood5, or bleeding after menopause, require immediate medical attention, even if they occur only once. In such cases, it is important to consult a doctor for proper diagnosis, as early detection can improve the survival rate.
The following are some early warning signs of cancer in your body that you should not ignore.
Sudden weight loss without any changes in diet is a warning sign. This is a common sign in both men and women. Cancer causes the way your body burns energy leading to weight loss. Lack of appetite during this time is also a contributing factor. This is usually seen in cancers related to the pancreas, head, neck, lungs, and upper digestive system6.

Extreme tiredness that does not improve with rest may be a sign. Fatigue in cancer is often due to anaemia, inflammation in the body or changes in the metabolism and energy levels in the body. It can also affect the mind and emotions. It is common in both men and women. It can make you feel exhausted, lazy, and weak. This is common in breast cancer, ovarian cancer, lung cancer, etc7.

A new lump or thickened area under the skin, especially in the breast, neck, armpit, or groin, should be checked. These may indicate abnormal cell growth or swollen lymph nodes. Commonly, swollen lymph nodes are caused by infections in which case they are usually soft and tender. However, lymph nodes that are hard, non-tender, fixed, and continue to grow may be a sign of cancer8. Lumps can be seen in both men and women. A lump in the breast, related to breast cancer, is more likely to occur in women than in men3.

Unusual bleeding, even if you are not hurt, can be a sign of cancer. It can occur in different parts of the body and can be seen in both men and women. Bleeding may appear as vomiting blood (haematemesis), coughing up blood (haemoptysis), or blood in the stool (melena or haematochezia), depending on where it comes from in the body. In women, abnormal bleeding from the vagina or breast may be seen in vaginal or breast cancer9,10. In men, blood in the urine or semen may be associated with prostate cancer11. The blood can appear red, brown or black.

Developing new moles or changes in existing moles, such as in their size, shape, colour (also yellowing of the skin) or texture, or itching, oozing or bleeding from them, are all signs to note. Any non-healing ulcers, skin or nail changes, should not be ignored9. These can be seen in both men and women. These changes are normally signs of skin cancer12.

Ongoing pain without a clear cause that does not improve over time may sometimes indicate cancer, especially if the pain continues for a long period, keeps coming back or gets worse9. Younger people have greater chances of developing more pain compared to adults13. It can be seen in men and in women.

A cough lasting for weeks, coughing up blood, or persistent hoarseness should not be ignored5,14. Coughing up blood (haemoptysis) alone is a serious warning sign and requires prompt medical evaluation. These symptoms can be seen in both men and in women. Such symptoms are normally seen in lung and throat cancer5,14.

Persistent changes in bowel movements are also warning signs to note. These include changes in bowel habits such as diarrhoea, constipation, or more frequent bowel movements, which lasts more than a few days (above 2-3 weeks). These habits are more seen in colorectal (bowel) cancer, as it affects the parts of the digestive system, colon and rectum15 and are seen in men and in women.

Persistent problems such as a sudden urge to urinate, differences in urine stream, frequent urination (particularly at night), pain or burning while urinating, etc., should not be ignored. These signs are common in men. They can occur in prostate cancer11.

Unexplained fever or sweats, particularly at night, may be the warning signs of cancer. These can occur in certain types of cancers, such as lymphoma (particularly night sweat), bone cancer, prostate cancer, leukaemia, etc16. However, these symptoms are not specific and can also be related to certain medications or infections9. In women, increased sweating may also be seen during menopause16.

A persistent feeling of heartburn or discomfort, or pain in the chest, and difficulty in swallowing, causing pain and burning, are the signs that should be taken into consideration9. They can occur in both men and women. These are the signs suggestive of throat cancer, lung cancer and bowel cancer5,14,15.
Early detection of cancer is very important because:
The following are some blood tests that can help detect cancer19:
Note: Screening and early detection methods have certain limitations, including false-positive results (when a test indicates cancer that is not present in real), false-negative results (when cancer is missed), and overdiagnosis (detection of cancers that may not cause harm). A combination of tests, including imaging and blood tests, is generally needed for confirmation.
Also Read: Types of Cancer: Symptoms, Early Signs, Diagnosis & More
You should consider consulting a doctor in the following situations:
People with higher risk factors, including older age, family or personal history of cancer, long-term tobacco or alcohol use, or chronic illnesses, specifically should seek timely medical advice if they notice any unusual or persistent changes18,19.
Also Read: Breast Cancer: Foods to Have and Avoid During and After Treatment
Cancer can often be treated more effectively when detected early. Warning signs like unexplained weight loss, fatigue, lumps, or unusual bleeding should not be ignored. Although these symptoms may not always mean cancer, they can still indicate changes in the body that need attention. Early medical consultation helps in timely diagnosis, better treatment, and improved recovery chances.
Also Read: Is Cancer a Genetic Disease? Hereditary Risk & Genetic Testing Guide
Only about 5-10% of cancer cases are caused by inherited genetic defects. About 90-95% are linked to environmental and lifestyle factors such as smoking, unhealthy diet, alcohol use, excessive sun exposure, pollution, infections, stress, obesity, etc20.
Cancer starts when normal cells in the body undergo changes (mutations) in their DNA. These changes cause the cells to grow and divide uncontrollably instead of following normal growth patterns. Over time, these abnormal cells can form a mass (tumour) and may spread to other parts of the body4.
Cancer lumps are usually poorly defined, irregular in shape, and may have lobulated edges. They may be me hard, fixed to tissues below and can gradually grow in size over time21.
Cancer often first shows up as small, unusual changes in the body such as a lump, unexplained weight loss, or persistent fatigue. These early signs are usually mild and may slowly worsen over time4,9.
The best anti-cancer foods, or cancer-fighting foods, include berries (raspberries, blackberries, blueberries, etc.), other fruits (bananas, citrus fruits, etc.), whole grains (whole-wheat pasta, raisin bran, barley, oatmeal, etc.), legumes (lentils, black beans, split peas, lima beans, baked beans, etc.) and vegetables (broccoli, spinach, dark green leafy vegetables, peas, etc.)22.
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Cancer is one of the major health problems around the world, affecting millions of people every year. Even though there is a big advancement in the medical treatment, many cases are detected very late, making the treatment procedure difficult. This is why knowing cancer is important, especially its early signs and symptoms. Finding cancer early can greatly improve the chances of successful treatment and recovery1.
There are different types of cancer, which can affect different body parts, and the early symptoms are often not clear or easy to notice. Common warning signs may include unexplained weight loss, constant tiredness, unusual lumps, unusual sweeting, etc2. Pain is usually a late feature in many cancers, so paying attention to the other changes in the body and consulting a doctor on time is important for diagnosis and improving treatment outcomes.
This article might help you understand the main types of cancer, their early warning signs and how they are diagnosed. The aim is to raise awareness, help detect cancers early, and encourage people to take better care of their health.
Cancer is a disease that happens when normal cells in the body change and start growing uncontrollably, forming a tumour that can spread and harm healthy tissues1. However, all tumours are not cancers. They can be benign or malignant3. Also, not all cancers form solid tumours, such as blood cancers, which have no discrete growth as such4.
The spread of cancer cells from one part of the body to another through the blood or lymph system is called metastasis. In addition, cancer also spread directly into nearby tissues (local invasion)3 or within body cavities, such as the abdomen6.
The risk of cancer increases with age. This is because, over time, the body builds up more risk factors, and the natural repair system of cells becomes less effective as we grow older1. Other risk factors include family history, lifestyle (smoking, alcohol, etc.), viral infections (human papilloma or hepatitis), etc2.
Cancer develops differently in each person, and not all growths are harmful. With early detection and proper treatment, many cancers can be managed effectively1.
There are different types of cancers which can develop in different body parts. Most of these cancers have very few known causes4,7,9. The following might help you understand how many types of cancer exist based on the types of cancer cells.
Carcinoma is a type of cancer that starts in epithelial tissue, which covers the skin and lines the inside of organs and body passages. It can develop in tissues that produce or secrete substances, such as in the breast, lungs, colon, prostate, or bladder, (adenocarcinoma) or in flat, thin cells that form the skin surface and line some internal organs (squamous cell carcinoma)10. The common cause is the accumulation of genetic changes over time, which leads cells to uncontrolled growth of cells. The risk factors that can trigger these genetic alterations including smoking, alcohol consumption, chemical exposure, lack of physical activity, obesity, etc11,12.
Sarcoma is a type of cancer that begins in the body’s supportive and connective tissues like bones, muscles, fat, cartilage, and tendons. It is more common in children and in adolescents, compared to carcinoma. However, several other types (soft tissue sarcomas) can also occur in adults. It often appears as a painful lump, especially in the bones, and the tumour usually looks like the normal tissue from where it starts10. It is commonly caused by mutation in the gene due to exposure to radiation or by certain cancer-causing chemicals (carcinogens)9.
Leukaemia is a blood cancer that begins in the bone marrow, the place where blood cells are produced. It disrupts the normal functioning of bone marrow, leading to the reduced production of red blood cells and the platelet count. This can cause problems like fatigue, anaemia, and poor blood clotting10. The risk factors include family history, age and sex, exposure to harmful radiations and chemicals, and viral infections (human T-cell leukaemia virus)4.
Myeloma (multiple myeloma) is a type of cancer that affects plasma cells, which are white blood cells that help fight infection by making antibodies8. The plasma cells produce certain types of protein (monoclonal (M) protein/paraprotein) which are found in the blood10. Here, abnormal plasma cells grow too much in the bone marrow and replace healthy blood cells, affecting red cells, white cells, and platelets. The risk factors include age, exposure to x-rays or other radiations, people belonging to specific races, etc8.
Lymphoma is a type of cancer that starts in the lymphatic system, which includes lymph nodes, spleen, tonsils, and thymus. This system helps fight infections by supporting the development and activation of white blood cells. It is a type of blood-related (hematologic) cancer, that is often seen as enlarged lymph nodes or mass-like growths. It can also develop in organs like the stomach, breast, or brain10. People with weak immune systems, those on immune-suppressing medicines, Epstein-Barr virus infection, radiation exposure, and those with a family history are at higher risk of developing lymphoma7.
There are several types of cancers. Below are some common types and their symptoms.
Although different types of cancer show different signs and symptoms, there are some warning signs to watch out for. The following are some early signs of cancer that you should not ignore.
Early detection of cancer plays a crucial role in improving outcomes and saving lives. The following says why early detection matters and how it is helpful to patients.
Note: Early detection helps improve outcomes in many cancers like breast, cervical, and colorectal cancer, but it is not equally effective for all cancers. Some, like pancreatic cancer, are often found late, while others (e.g., prostate or thyroid cancer) may be over diagnosed. Early treatment can improve well-being but may still cause side effects, and even advanced cancers can sometimes be managed with good care.
The following is a list of blood tests performed in early cancer detection.
Note: Diagnosis of cancer typically requires histopathological confirmation (biopsy); imaging or basic blood screening tests alone are generally not definitive for most cancers.
You should consider seeing a doctor if you notice:
Also Read: Does Masturbating Increase Risk of Prostate Cancer or Vice Versa?
Cancer is a serious condition, but it can often be effectively managed, especially with early detection. Recognising warning signs and going for regular check-ups can greatly improve treatment outcomes. Understanding different types of cancer and their symptoms helps you stay aware and take timely action. Prioritising your health and consulting a doctor when needed can make a life-saving difference.
An MRI cannot test all types of cancer. It is good to detect cancer caused in the brain, soft tissues, breast and colon12,14,21. However, it has limitations in early diagnosis of some types of cancers like lung cancer21.
There are said to be more than 200 types of cancer which affect the organs, tissues, blood, bone marrow and immune system2.
Yes, it is possible for a person to have more than one type of cancer, either at the same time or one after another. This is called multiple primary cancers. Although it is not very common, these cancers start separately in different parts of the body and are not caused by the spread of an existing cancer22.
The silent signs of cancer include:
-Unexplained weight loss
-Lack of appetite
-New or unexplained pain2
-New mole or changes in existing mole (skin changes)
-Unusual bleeding or bruising
-Changes in bowel movement
-Long-term cough or hoarseness17
-Difficulty in breathing or swallowing, chest pain or discomfort, etc11
The most common types of cancer found in women are breast cancer, cervical cancer, ovarian cancer, uterine cancer, oral cancer and colorectal cancer23.
The most common types of cancer found in men are prostate cancer, colorectal cancer, lung cancer, oral cancer, stomach cancer and oesophageal cancer23.
1. Cancer. 2025. Doi: https://www.who.int/news-room/fact-sheets/detail/cancer
2. Cancer: NHS. 2025. Doi: https://www.nhs.uk/conditions/cancer/
3. Cancer: Medline. 2025. Doi: https://medlineplus.gov/cancer.html
4. Leukaemia. 2023. Doi: https://www.healthdirect.gov.au/leukaemia
5. Benign. 2025. Doi: https://medlineplus.gov/ency/article/002236.htm
6. Menon G, Santillan VR. Peritoneal Surface Malignancies. 2025. Doi: https://www.ncbi.nlm.nih.gov/books/NBK541114/
7. Lymphoma. 2025. Doi: https://www.healthdirect.gov.au/lymphoma
8. Myeloma Basics. 2025. Doi: https://www.cdc.gov/myeloma/about/index.html
9. Causes, Risk Factors, and Prevention of Soft Tissue Sarcomas. 2026. Doi: https://www.cancer.org/cancer/types/soft-tissue-sarcoma/causes-risks-prevention.html
10. Cancer Classification. Doi: https://training.seer.cancer.gov/disease/categories/classification.html
11. Lung Cancer. 2025. Doi: https://medlineplus.gov/lungcancer.html
12. Breast Cancer. 2025. Doi: https://medlineplus.gov/breastcancer.html
13. Colorectal Cancer. 2024. Doi: https://medlineplus.gov/colorectalcancer.html
14. Bowel cancer (colon and rectal cancer). 2023. Doi: https://www.healthdirect.gov.au/bowel-cancer
15. Prostate Cancer. 2024. Doi: https://medlineplus.gov/prostatecancer.html
16. Sathe NC, Zito PM. Skin Cancer. 2025. Doi: https://www.ncbi.nlm.nih.gov/books/NBK441949/
17. Symptoms of Cancer. 2019. Doi: https://www.cancer.gov/about-cancer/diagnosis-staging/symptoms
18. Imai M, Nakamura Y, Yoshino T. Transforming cancer screening: the potential of multi-cancer early detection (MCED) technologies. Int J Clin Oncol. 2025;30(2):180-193. doi:10.1007/s10147-025-02694-5. https://pubmed.ncbi.nlm.nih.gov/39799530/
19. Tumor Marker Tests in Common Use. 2023. Doi: https://www.cancer.gov/about-cancer/diagnosis-staging/diagnosis/tumor-markers-list
20. How Cancer Is Diagnosed. 2023. Doi: https://www.cancer.gov/about-cancer/diagnosis-staging/diagnosis
21. Sim AJ, Kaza E, Singer L, Rosenberg SA. A review of the role of MRI in diagnosis and treatment of early stage lung cancer. Clinical and Translational Radiation Oncology. 2020;24:16-22. doi:10.1016/j.ctro.2020.06.002. https://pmc.ncbi.nlm.nih.gov/articles/PMC7306507/
22. Vogt A, Schmid S, Heinimann K, et al. Multiple primary tumours: challenges and approaches, a review. ESMO Open. 2017;2(2):e000172. doi:10.1136/esmoopen-2017-000172. https://www.esmoopen.com/article/S2059-7029(20)32451-0/fulltext
23. Kalra K. Common Cancers in India, theirincreasing incidence. Symptomswhich need immediate attention. Doi: https://www.cghs.mohfw.gov.in/CGHSGrievance/FormFlowXACTION?hmode=ftpFileDownload&fileName=23052025114829_Common-Cancers-in-India-their-increasing-incidence-(9-November-2021)-.pdf&folderName=Circular&isGlobal=1
24. Nicholson BD, Hamilton W, O’Sullivan J, Aveyard P, Hobbs FR. Weight loss as a predictor of cancer in primary care: a systematic review and meta-analysis. Br J Gen Pract. 2018;68(670):e311-e322. doi:10.3399/bjgp18X695801. https://pubmed.ncbi.nlm.nih.gov/29632004/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.