You’ve probably heard of this disclaimer on multiple occasions – ‘smoking is injurious to health’. What you may not immediately realise is the extent of the damage smoking can cause to your health and, most directly, your lungs.
Smoking is known to be the leading cause of preventable diseases and deaths globally. Nearly all forms of lung cancer, the top cause of cancer death in both men and women, can be attributed to smoking. Tobacco and tobacco-related products can damage the lungs’ ability to supply oxygen to the body. Other substances commonly found in cigarette smoke can cause permanent lung damage, even in small amounts.
A single puff of cigarette smoke contains upwards of 7,000 chemicals. Tobacco smoke contains over 70 known cancer-causing chemicals2. When you breathe these in, these toxins go deep into your lungs and can cause swelling, resulting in a host of other respiratory diseases.
Both tobacco and chemical substances found in cigarettes can change the cellular structure of the lungs. They can cause the elastic walls within the airways to break down – resulting in less functioning surface area in the lungs. Cigarettes can damage lung tissue, preventing them from functioning correctly. This can increase the risk of diseases caused by smoking, such as chronic bronchitis, emphysema, respiratory diseases, asthma and COPD (Chronic Obstructive Pulmonary Disease)1.
Nicotine in tobacco can also damage the ability of the respiratory system to filter out dust and dirt. This can lead to toxic substances passing through, resulting in lung congestion and the ‘smoker’s cough’.
Also Read: What Is Hantavirus? Symptoms, Causes, & Effective Prevention
A person who smokes throughout life is at high risk of developing a range of potentially fatal diseases owing to impaired lung function and breathlessness due to swelling and narrowing of the lung airways and excess mucus build-up. They are also prone to weakening the lungs’ clearance system, leading to the accumulation of toxic substances and causing lung irritation and damage. Further, they are also at an increased risk of lung infection, chronic bronchitis and heightened risk of asthma, along with permanent damage to air sacs3.
In the longer term, smoking is known to induce heart disease and stroke, in certain cases, it can cause ulcers of the digestive system and put smokers at increased risk of type 2 diabetes.
Most smokers are also likely to develop emphysema. The number of cigarettes you smoke and other lifestyle factors may impact the extent of the damage. If you’re diagnosed with either of these respiratory diseases – emphysema or chronic bronchitis, you run the risk of being diagnosed with chronic obstructive pulmonary disease (COPD).
Also Read: Does Smoking Really Affect Your Brain?
Smoking can affect a person’s health in other ways, too, harming almost every organ in the body. In most cases, it can result in a compromised immune system function, making you susceptible to many other illnesses. It can also lead to lower bone density (brittle bones), which increases the risk of broken bones and fractures. Smoking also leaves you at a higher risk of rheumatoid arthritis, heart disease and stroke, along with an increased risk for cataracts (clouding of the eye lenses).
Apart from respiratory diseases, other visible disorders include an increased risk of oral cancers, gum disease and tooth loss, premature ageing of the skin, bad breath and stained teeth and an increased risk for age-related macular degeneration, which can lead to blindness. Moreover, even your wounds may take longer to heal!
Also Read: 6 Simple Exercises to Improve Your Lung Health
It’s never too late to quit smoking. Within days of quitting smoking, lungs begin to repair themselves. In fact, just 12 hours after you quit, the amount of carbon monoxide in your blood drops to a much healthier level. More oxygen flows to your vital organs and you will be able to breathe better. In about 10 to 15 years, your risk of developing lung cancer reduces and may even become the same as a non-smoker4.
Also Read: How to Avoid Asthma Attacks During Winter
1. Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2010. 7, Pulmonary Diseases. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53021/
2. National Cancer Institute. Harms of Cigarette Smoking and Health Benefits of Quitting [Internet]. Bethesda (MD): National Cancer Institute; reviewed 19 December 2017 [cited 2025 Sep 19]. Available from: https://www.cancer.gov/about-cancer/causes-prevention/risk/tobacco/cessation-fact-sheet
3. Varghese J, Muntode Gharde P. A Comprehensive Review on the Impacts of Smoking on the Health of an Individual. Cureus. 2023 Oct 5;15(10):e46532. doi: 10.7759/cureus.46532. PMID: 37927763; PMCID: PMC10625450. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10625450/
4. Centers for Disease Control and Prevention. Benefits of Quitting Smoking [Internet]. Atlanta (GA): CDC; updated May 15, 2024 [cited 2025 Sep 19]. Available from: https://www.cdc.gov/tobacco/about/benefits-of-quitting.html
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
 10
10

31st May is known as the ”World No Tobacco Day” and for a good reason too1. Did you know that more than 10 million die each year in India due to tobacco? India is home to 12% of the world’s smokers, according to the World Health Organization (WHO). You have heard numerous people tell you that smoking affects your lungs. You have seen the gross pictures on cigarette packs but smoked anyway. But did you know that smoking affects your brain too?
Nicotine works like the various neurotransmitters that are already there in our brain. It activates dopamine signals that result in a pleasant sensation in your brain. With the passing of time and more smoking, the brain reduces acetylcholine receptors to compensate for the increased signalling activity. As a result, nicotine tolerance is created in the brain2.
The brain ends up needing more nicotine. As nicotine mimics the work of dopamine that provides the feel-good factor, your brain starts associating smoking (nicotine use) with feeling good. The nicotine in cigarettes changes your brain and makes you suffer from withdrawal symptoms when you try to quit. You start feeling irritable, anxious, and your body has a strong craving for nicotine. As a result of these symptoms, most people reach for another cigarette, and then another and are unable to quit.

Brain size and volume is associated with higher intelligence and better cognitive functioning. The average brain volume in adult males is 1260 cubic cm and 1130 cubic cm in adult females. According to a 2017 study2, the longer you smoke, the more your brain loses volume with vital tissues shrivelling up.
Smoking affects the subcortical brain regions. The subcortical areas of the brain are associated with pleasure, hormone production, emotion, and memory. Smokers thus develop age-related loss of brain volume that leads to an increased risk of dementia and is one of the ways how smoking harms the brain.

Dementia is a syndrome that is characterized by deterioration in thinking, memory, behaviour, and the ability to perform everyday activities. It is said to affect older people mainly, but it is not a normal part of ageing. Since smoking affects the subcortical regions of the brain that are associated with memory, it puts smokers at a higher risk of dementia.
In 2015, a research team reviewed 37 studies that compared smokers and non-smokers and found that smokers were 30 % more likely to be affected by dementia. Quitting smoking can decrease the risk of dementia in the person4.
Cigarette smoking has been associated with dementia and dementia-related brain changes, notably gray matter (GM) volume atrophy. These associations are thought to reflect the co-morbidity of smoking and vascular, respiratory, and substance use/psychological conditions.
Dr. M.G. Kartheeka, MBBS, MD(Pediatrics)

One of the smoking effects on brain is cognitive decline, which usually happens as people get older. But in smokers, it starts much earlier. Signs and symptoms of cognitive decline include:
In 2012, the cognitive data of about 7,000 men and women were studied for 12 years. The researchers found that smokers experienced a much more rapid cognitive decline than non-smokers. Middle-aged male smokers were found to be more at risk than female smokers4.

If you smoke say, 20 cigarettes a day, you are 6 times more likely to have a stroke than a non-smoker. Tobacco contains over 7,000 harmful chemicals, including formaldehyde, cyanide, arsenic, and carbon monoxide. These toxic chemicals get transferred from the lungs to the blood. They make platelets more likely to stick together. Platelets help in clotting the blood in case of blood loss, but if the platelets stick together, it increases the chance of clot-forming5.
Smokers are at a higher risk of developing atherosclerosis where arteries become hardened and narrow. It restricts smooth blood flow making the formation of blood clots more likely. If a clot forms in an artery leading to the brain, it can block the blood supply to a part of the brain resulting in a stroke. This is known as ischaemic stroke. Smoking is said to double the risk of having an ischaemic stroke. If a person quits smoking, within 5 years, his/her risk of stroke will start decreasing to that of a non-smoker.

Smoking releases a severe amount of toxicity in our bodies. There are about 60 known cancer-causing substances in tobacco6. The chemicals that make up a cigarette are:
Smoking also causes a temporary spike in blood pressure, which can weaken the arterial walls and make them more prone to form an aneurysm and rupture. The harmful chemicals in a cigarette are also implicated in the causation of brain cancer.
Dr. Ashish Bajaj, M.B.B.S., M.D. in Clinical Pharmacology and Toxicology

Smoking affects the brain and hence, mental health. Sometimes, bad mental health makes people take up smoking and worsen their conditions. Other times, it is the other way around7.

The nicotine from cigarettes alters the brain. It makes the brain connect ‘feeling good’ to smoking. Quitting smoking becomes tough after some time because smokers start suffering from withdrawal symptoms. They then find solace in smoking and fall prey to the dangerous cycle and become addicted.

How many times have you heard somebody say, ‘I’m feeling stressed out, I need to smoke right now’ or ‘Smoking makes me feel relaxed’7?
Stress is very common and can cause symptoms like headaches, irritability, anxiety, and/or breathlessness at times. Smoking increases the occurrence of these symptoms. Smokers start feeling the symptoms if they do not smoke for a long time and associate smoking with being a reliever of stress.

Nicotine mimics the work of dopamine, prompting the brain to switch off its mechanism that makes and secretes dopamine. In the long term, the supply of dopamine decreases in the brain and inspires people to smoke more. There is a complex relationship between depression and smoking. Smokers with depression have more trouble quitting as withdrawal symptoms become more severe in them7.

Research has shown smoking increases tension and anxiety. The relaxed feeling that smokers talk about after a quick smoke fades away just as quickly. It is hugely short-lived and only adds more jitteriness in the smoker, making him/her reach for more7.

It has been reported that people who suffer from a serious mental disorder known as Schizophrenia tend to be heavy smokers. Some people suffering from this disorder have claimed that smoking helps them to numb the debilitating symptoms of schizophrenia and also to mitigate the side effects experienced from the medication for the same. Ironically, recent research has found that excessive smoking may very well be one of the causes for the onset of schizophrenia. However, since there is more research required to fully confirm this, it has not yet received mainstream acceptance. Nevertheless, it is best to avoid smoking to reduce the risk of developing such mental disorders8.
Yes, e-cigarettes have negative effects on the brain too. National Institute on Drug Abuse has reported that the nicotine in e-cigarettes goes about making similar harmful changes in the brain. E-cigarette vapour contains harmful chemicals too hence it is not a way out.
If all this information on how smoking affects the brain has you worried, you can always try quitting. Most addictions are hard to overcome. But since smoking has been around for a while there are well-established methods to try out. Keep in mind, since everyone is different not all approaches will work the same for you. Some may be more effective than others, do what works best for you9.
Absolutely! Within 20 minutes of quitting smoking, your heart rate will slow down. Within 12 hours, levels of carbon monoxide in your blood will start decreasing. Within 3 months, lung functions and blood circulation will start getting better. Within a year of quitting, your risk of having a heart attack will start decreasing by a whopping 50 %. Within 5 to 15 years, your risk of suffering a stroke will reduce to that of a non-smoker.
Also Read: What Happens To Your Lungs From Smoking? Things You Should Know
1. World Health Organization. World No Tobacco Day – 31 May is World No Tobacco Day [Internet]. Geneva: WHO; [cited 2025 Dec 5]. Available from: https://www.who.int/campaigns/world-no-tobacco-day
2. Valentine G, Sofuoglu M. Cognitive Effects of Nicotine: Recent Progress. Curr Neuropharmacol. 2018;16(4):403-414. doi: 10.2174/1570159X15666171103152136. PMID: 29110618; PMCID: PMC6018192. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6018192/
3. Chang Y, Thornton V, Chaloemtoem A, Anokhin AP, Bijsterbosch J, Bogdan R, Hancock DB, Johnson EO, Bierut LJ. Investigating the Relationship Between Smoking Behavior and Global Brain Volume. Biol Psychiatry Glob Open Sci. 2023 Oct 6;4(1):74-82. doi: 10.1016/j.bpsgos.2023.09.006. PMID: 38130847; PMCID: PMC10733671. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10733671/
4. Peters R, Poulter R, Warner J, Beckett N, Burch L, Bulpitt C. Smoking, dementia and cognitive decline in the elderly, a systematic review. BMC Geriatr. 2008 Dec 23;8:36. doi: 10.1186/1471-2318-8-36. PMID: 19105840; PMCID: PMC2642819. Available from:https://pmc.ncbi.nlm.nih.gov/articles/PMC2642819/
5. Shah RS, Cole JW. Smoking and stroke: the more you smoke the more you stroke. Expert Rev Cardiovasc Ther. 2010 Jul;8(7):917-32. doi: 10.1586/erc.10.56. PMID: 20602553; PMCID: PMC2928253. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2928253/
6. Vida S, Richardson L, Cardis E, Krewski D, McBride M, Parent ME, Abrahamowicz M, Leffondré K, Siemiatycki J. Brain tumours and cigarette smoking: analysis of the INTERPHONE Canada case-control study. Environ Health. 2014 Jun 27;13:55. doi: 10.1186/1476-069X-13-55. PMID: 24972852; PMCID: PMC4088305. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4088305/
7. Boksa P. Smoking, psychiatric illness and the brain. J Psychiatry Neurosci. 2017 May;42(3):147-149. doi: 10.1503/jpn.170060. PMID: 28440208; PMCID: PMC5403659. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5403659/
8. Ding JB, Hu K. Cigarette Smoking and Schizophrenia: Etiology, Clinical, Pharmacological, and Treatment Implications. Schizophr Res Treatment. 2021 Dec 13;2021:7698030. doi: 10.1155/2021/7698030. PMID: 34938579; PMCID: PMC8687814. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8687814/
9. Centers for Disease Control and Prevention. Tips For Quitting. Tips From Former Smokers. 2024 Sept 27 [cited 2025 Dec 05]. Available from: https://www.cdc.gov/tobacco/campaign/tips/quit-smoking/tips-for-quitting/index.html
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
20
2
Skin concerns, such as itchy rashes, unexplained skin irritation, or discomfort that keeps coming back, could be quite bothersome. Some skin conditions may be linked to underlying health issues and require proper evaluation.
Dermatitis herpetiformis is a long-term, very itchy skin condition that causes small blisters, bumps, and sore patches. It happens when the immune system reacts to gluten, and this reaction affects the skin1,2.
Understanding dermatitis herpetiformis causes, its symptoms, and the treatments involved may help individuals detect and manage this condition early and effectively.
Dermatitis herpetiformis, also as Duhring disease, is a long-lasting autoimmune skin condition. It usually causes an intensely itchy rash with small bumps or blisters on both sides of the limbs and body, especially on the elbows, knees, buttocks, scalp, and back3. Because the blisters are often scratched, a person may notice scabs, scratches, or sore areas instead of clear blisters1.
Dermatitis herpetiformis symptoms include,2:
Dermatitis herpetiformis causes:
Some individuals are more vulnerable to getting Dermatitis Herpetiformis than others. These include:
If untreated or poorly managed, dermatitis herpetiformis can progress into more serious conditions, as follows:
A doctor may diagnose dermatitis herpetiformis using the following tests and assessments:
Treatment for dermatitis herpetiformis usually focuses on a strict gluten-free diet for long-term control. Because gluten can be hidden in many foods. It is helpful to consult a dietitian before making major diet changes. The rash may take months or longer to improve after starting a gluten-free diet, so some people may also need medications for symptomatic relief1. Treatment may include:

A gluten-free diet removes foods that contain wheat, barley, and rye. Some people may also need to avoid oats unless they are certified gluten-free and approved by their healthcare team4.

Doctors may prescribe medicines such as dapsone or other options to reduce itching and blisters. These medicines need medical supervision and monitoring for side effects1.

Avoid exposure to iodine-containing foods/medications, as it can trigger dermatitis herpetiformis symptoms1.
Dermatitis herpetiformis does not have a known prevention. Prevention of the complications of the condition could include the following1:
Also Read: Typhoid Fever Rash: When Rose Spots Appear & What You Should Do
Dermatitis herpetiformis is a long-term skin condition linked to gluten sensitivity and coeliac disease. It can cause severe itching, small blisters, and sore or scratched skin. A strict gluten-free diet is the main long-term treatment, and medicines may help control symptoms while the diet takes effect. Anyone with a persistent, very itchy rash should speak with a healthcare professional for proper testing and treatment.
With the right diagnosis, medical follow-up, and diet support, many people can reduce flare-ups and lower the risk of related complications.
Dermatitis herpetiformis is associated with severe itching, scars, skin erosions, and a rash that is symmetrical on the back, buttocks, knees, and elbows. It is similar to the rash in eczema2.
Sensitivity to gluten and gliadin (a derivative of gluten) can cause the characteristic rash suggestive of dermatitis herpetiformis, which could be diagnosed through physical examination, blood tests, and a skin biopsy1,7.
Yes, it could occur at any time in life, depending on the extent of exposure to gluten, the immunity at the time, and the overall health of the individual. It is often seen in individuals who are 15 to 40 years old4,8.
No, dermatitis herpetiformis is not contagious. It is an autoimmune, lifelong condition that affects the skin and could be hereditary. It is not an infection that could spread from one person to another9.
Even though the name may suggest herpes, it has no relevance to the herpes virus, and it is an autoimmune condition where the immune cells fail to recognise their own cells2.
Excess alcohol intake could make an individual more sensitive to gluten, particularly if a close family relative is known to have dermatitis herpetiformis. In an individual already diagnosed with the condition, alcohol intake could worsen the symptoms1,10.
No, stress is not known to cause dermatitis herpetiformis. It is mainly caused by immune sensitivity to gluten1.
Yes, the rash in dermatitis herpetiformis may seem like acne because it also appears like a small, papular lesion. However, it also looks similar to an eczema rash. Therefore, simple visual diagnosis is challenging2.
1. Mirza HA, Gharbi A, Bhutta BS. Dermatitis Herpetiformis. In: StatPearls. StatPearls Publishing; 2026. Accessed July 28, 2026. Available from: http://www.ncbi.nlm.nih.gov/books/NBK493163/
2. Dermatitis herpetiformis: MedlinePlus Medical Encyclopedia. Accessed July 28, 2026. Available from: https://medlineplus.gov/ency/article/001480.htm
3. Nguyen CN, Kim SJ. Dermatitis Herpetiformis: An Update on Diagnosis, Disease Monitoring, and Management. Medicina (Mex). 2021;57(8):843. doi:10.3390/medicina57080843 Available from: https://pubmed.ncbi.nlm.nih.gov/34441049/
4. Dermatitis herpetiformis symptoms and treatments. NHS inform. Accessed July 28, 2026. Available from: https://www.nhsinform.scot/illnesses-and-conditions/skin/rashes-irritation-and-swelling/dermatitis-herpetiformis/
5. Reunala T, Hervonen K, Salmi T. Dermatitis Herpetiformis: An Update on Diagnosis and Management. Am J Clin Dermatol. 2021;22(3):329-338. doi:10.1007/s40257-020-00584-2 Available from: https://pubmed.ncbi.nlm.nih.gov/33432477/
6. Dermatitis Herpetiformis – NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. Accessed July 28, 2026. Available from: https://www.niddk.nih.gov/health-information/professionals/clinical-tools-patient-management/digestive-diseases/dermatitis-herpetiformis
7. Collin P, Salmi TT, Hervonen K, Kaukinen K, Reunala T. Dermatitis herpetiformis: a cutaneous manifestation of coeliac disease. Ann Med. 2017;49(1):23-31. doi:10.1080/07853890.2016.1222450 Available from: https://pubmed.ncbi.nlm.nih.gov/27499257/
8. Reunala T, Hervonen K, Salmi T. Dermatitis Herpetiformis: An Update on Diagnosis and Management. Am J Clin Dermatol. 2021;22(3):329-338. doi:10.1007/s40257-020-00584-2 Available from: https://pubmed.ncbi.nlm.nih.gov/33432477/
9. Rybak-d’Obyrn J, Placek W. Etiopathogenesis of dermatitis herpetiformis. Adv Dermatol Allergol Dermatol Alergol. 2022;39(1):1-6. doi:10.5114/ada.2020.101637 Available from: https://pubmed.ncbi.nlm.nih.gov/35369614/
10. Currie S, Hoggard N, Clark MJR, et al. Alcohol Induces Sensitization to Gluten in Genetically Susceptible Individuals: A Case Control Study. PLoS ONE. 2013;8(10):e77638. doi:10.1371/journal.pone.0077638 Available from: https://pubmed.ncbi.nlm.nih.gov/24204900/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Imagine waking up one morning to realise that the vision in one eye has suddenly become blurred or unclear. These vision changes may be a sign of an eye stroke, an eye condition that requires quick medical attention.
Eye stroke is a condition that occurs when there is a blockage in the blood vessel of the retina, a light-sensitive tissue behind the eyes1.
Understanding what causes eye strokes, their symptoms, and their treatment may help individuals in the early detection and effective management of this condition.
An eye stroke is a serious medical condition that affects the eye. It is similar to a stroke affecting the brain and occurs when the central retinal artery or vein, the blood vessels that supply and drain the retina (the light-sensitive tissue at the back of the eye), become blocked due to a blood clot or fatty deposit1,4. Retinal nerve damage could occur if blood supply is not restored promptly. An eye stroke is more frequently observed in people with conditions affecting the blood vessels1.
The retina receives oxygen and nutrients mainly through the central retinal artery and the choriocapillaris blood vessels. When the central retinal artery becomes blocked, the retina does not receive enough oxygen and nutrients. If blood flow is not restored promptly, the retinal cells can become damaged within a short time. This can lead to sudden, painless vision loss, known as an eye stroke, which requires immediate medical attention. Similarly, individuals with central retinal vein occlusion (blockage) may experience blurring or loss of vision in the affected eye.
If the blockage that causes the eye stroke is not treated promptly, there may be vision loss that may not be reversible, which is of serious concern5.
Loss of vision in one eye (full or part loss of vision) is a characteristic symptom of a stroke in eye2. Eye stroke symptoms include3,6:
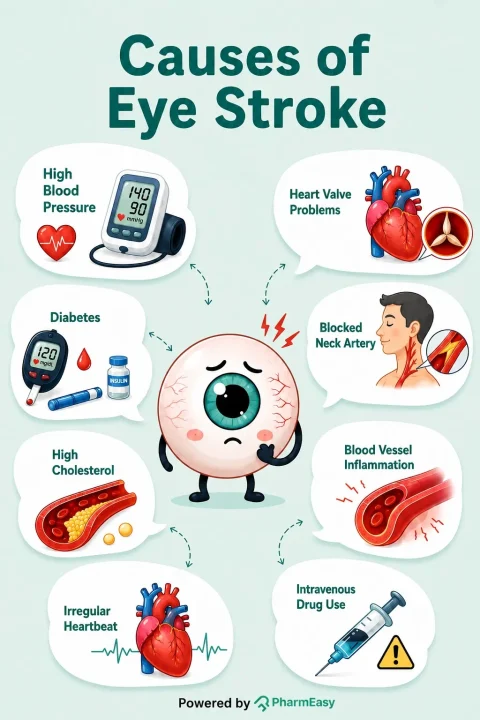
Stroke in eye may mainly occur due to disruption of the blood flow through the central retinal artery or vein due to its blockage by fat, calcium, or blood clot2,3,5. Eye stroke causes include2:
Eye stroke treatment includes various techniques to restore blood flow to the eye. However, treatment options are limited, and vision may not fully recover, especially when a large retinal area is involved. Time is critical, and treatment should be initiated as soon as possible. Studies suggest that treatment should be initiated within 2 to 4 hours of symptom onset2,5. Eye stroke treatment includes:

Measures to avoid an eye stroke include managing the conditions that affect the blood vessels, such as coronary artery disease2. This involves:
An eye stroke is a medical emergency, and you must seek prompt medical attention if you experience symptoms such as blurring or vision loss. If you are at risk of heart or blood vessel conditions, it is advised to routinely evaluate your vision as early detection can help in preserving your vision5.
Also Read: Could Yellow Eyes Be Serious? Causes, Symptoms & Treatment Guide
An eye stroke could happen suddenly without any warning. However, prompt intervention can play a significant role in treatment outcomes to protect the vision. Never ignore symptoms such as sudden vision loss, dark spots or blurring of vision, as they may require quick medical attention. Early diagnosis and adequate treatment could help to preserve the vision and detect any underlying medical condition that needs attention. If you or your dear ones experience any such eye stroke symptoms, seek swift emergency care, because when it comes to an eye stroke, every minute counts.
Also Read: What Is Eye Strain and How Can You Reduce It in the Digital Age
An eye stroke itself is not usually life-threatening. However, it may be a warning sign of underlying blood vessel disease and is associated with an increased risk of a brain stroke. Because both conditions share the same risk factors, prompt medical evaluation is essential6.
An eye stroke may cause permanent loss of vision, but the outcome depends on how severe the blockage is and how quickly treatment is started. Prompt treatment offers the best chance of preserving vision, although full recovery may not always be possible4,5.
Studies suggest a golden window for the treatment of eye stroke lies between 90 minutes and 4 hours from the beginning of symptoms however, full recovery may not always be possible8.
Stress alone may not directly cause an eye stroke; however, long-term stress may contribute to conditions such as high blood pressure and narrowing of blood vessels, which can increase the risk of an eye stroke9.
Eye stroke is quite rare, with data suggesting that around 1 in 10,000 people may experience it. It is also rarely reported in young individuals10.
An eye stroke does not directly lead to a brain stroke. However, it is associated with a higher risk of developing a brain stroke because both conditions share many of the same risk factors, such as high blood pressure and diabetes11.
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Many people, particularly young adults, want to gain muscle to feel stronger, improve fitness, or support healthy body goals1. However, building muscle takes more than exercise alone. Resistance training, along with a balanced muscle gain diet, gives the body the nutrients it needs to repair and build muscle after exercise. This repair process is often called muscle protein synthesis. Eating enough protein, carbohydrates, healthy fats, and other essential nutrients can support workout performance, muscle growth, and recovery2. This blog explains what a muscle gain diet is, the best foods to include, a simple 7-day meal plan, and practical nutrition tips to help you build muscle safely and effectively.
Muscles grow when the body repairs and builds new muscle tissue after exercise. Resistance training gives the muscles a reason to adapt, while nutrients from food provide the building blocks and energy needed for repair and growth. Protein intake and resistance exercise work together to support muscle development2.
Protein is important for muscle gain because it provides amino acids, which are the body’s building blocks for muscles. When you eat enough protein, your body is better able to repair muscle after exercise and builds new muscle tissue. Spreading protein across meals during the day may help provide a steady supply of amino acids for muscle recovery2. Diet also gives you the energy needed to exercise and recover. Carbohydrates help fuel workouts by supporting muscle glycogen, the stored form of carbohydrate used during exercise. After training, carbohydrates help refill these energy stores. Nutrient-rich foods, including milk and other good-quality protein sources, also provide vitamins and minerals that support muscle health3.
To build muscle, your body needs nutrients that help repair muscle, provide energy for training, and support recovery after workouts4,5.
Important nutrients for muscle gain include:
A varied diet that includes these nutrients can help your body respond well to resistance training and support long-term improvements in strength and muscle size4,5.
The best foods for muscle gain are foods that provide protein, energy, and other nutrients your body needs for training and recovery. Protein-rich foods are especially helpful because they provide amino acids for muscle repair and growth when combined with regular resistance exercise4,6.
Some of the best foods to gain muscle include:

Eggs are a good-quality protein source because they provide all the essential amino acids needed for muscle repair and growth.2 They also contain leucine, an amino acid that helps support the muscle-building process2,4.

Milk contains whey and casein proteins, which provide essential amino acids for muscle repair and growth. Having milk after exercise may help support recovery and refill energy stores when it is part of a balanced diet2,6.

Pulses such as lentils, chickpeas, green gram, kidney beans, and peas provide plant-based protein. Combining pulses with cereals improves the balance of essential amino acids6.

Fish, poultry, and lean meat provide complete proteins containing all essential amino acids required for muscle protein synthesis.

Nuts and seeds, including almonds, walnuts, chia seeds, pumpkin seeds, and flax seeds, provide plant-based protein and healthy fats.

Soybeans and soy products provide plant-based protein containing essential amino acids4,6.
A muscle gain diet should focus on nutritious foods most of the time. It is helpful to limit foods that are high in added fat, sugar, and salt, as well as many ultra-processed foods, because they may add calories without providing many important nutrients.
Some foods to limit during a muscle gain diet include:
Adding vitamins or minerals to ultra-processed foods does not make them as nutritious as fresh, minimally processed foods6.
A balanced 7-day meal plan for muscle gain should include enough protein, carbohydrates, healthy fats, and a variety of nutrient-rich foods. These may include cereals, pulses, dairy products, eggs, lean meat or fish, fruits, vegetables, nuts, and seeds. Together, these foods can support muscle growth, recovery, and overall nutrition needs4,6.
The table below provides a sample 7-day meal plan for muscle gain that can be adjusted according to individual calorie needs, dietary preferences, and training goals2,4,6:
| Day | Breakfast | Lunch | Snacks | Dinner |
| Day 1 | Oats with milk, banana and nuts | Brown rice, dal, vegetables, curd and salad | Fruit smoothie with milk | Chapati, paneer/tofu, vegetables and curd |
| Day 2 | Millet porridge with milk, boiled eggs and fruit | Whole grain rice, chickpea curry, green leafy vegetables and curd | Nuts, fruit and yoghurt | Chapati, fish/chicken curry, vegetables and salad |
| Day 3 | Whole wheat bread, eggs and milk | Roti, rajma, vegetables, curd and fruit | Banana with peanut butter or nuts | Rice, dal, vegetables and curd |
| Day 4 | Ragi dosa with sambar and milk | Millet rice, pulses, vegetables and curd | Fruit smoothie with yoghurt | Chapati with paneer/chicken and vegetables |
| Day 5 | Oatmeal with milk, nuts and seasonal fruit | Rice, fish/egg curry, vegetables and salad | Sprouts, nuts and fruit | Whole grain roti, dal, vegetables and curd |
| Day 6 | Idli with sambar, milk and fruit | Chapati, soybean/pulse curry, vegetables and curd | Milk with banana or homemade smoothie | Rice, lean meat/fish or pulses, vegetables and salad |
| Day 7 | Millet upma with vegetables, nuts and milk | Whole grain rice, dal, vegetables, curd and fruit | Boiled eggs or roasted chickpeas with fruit | Chapati, paneer/tofu or chicken, vegetables and curd |
This meal plan focuses on obtaining essential nutrients from a variety of foods rather than relying on excessive supplements, helping support muscle growth, energy levels, and recovery during trainin2,5,6
A gym diet plan for muscle gain should include the right foods before and after workouts to provide energy, support muscle repair, and improve recovery. The following sections explain what to eat before and after workouts:
| Meal | Sample foods |
| Breakfast | Oatmeal with a banana |
| Mid-morning snack | Low-fat yoghurt |
| Lunch | Whole-grain pasta |
| Pre-workout meal | Fruit smoothie made with low-fat milk |
| Post-workout meal | Whey protein shake with a banana |
| Dinner | Whole-grain cereal with milk |
| Bedtime snack | Fruits |
This is only a sample gym diet plan. You can change the foods and portion sizes to suit your daily routine, workout schedule, and personal food preferences5.

Building muscle is not only about diet. Healthy lifestyle habits also help your muscles recover, improve workout performance, and support steady progress over time. Important habits include:
Along with following a muscle gain diet, practising these healthy habits can help you build muscle more effectively and stay healthy.
Also Read: List of Protein Rich Food for Vegetarians
A well-planned muscle gain diet, combined with regular resistance training, can help support muscle growth, improve strength, and promote recovery. Focus on including high-quality protein, carbohydrates, healthy fats, and a variety of nutrient-rich whole foods instead of relying on supplements. Along with following a balanced diet, stay well hydrated, get enough sleep, manage stress, and avoid smoking and excessive alcohol consumption to support your muscle-building goals and overall health.
A balanced muscle gain diet that includes enough protein, carbohydrates, and healthy fats is best for supporting muscle growth and recovery. Protein helps repair and build muscle, while carbohydrates provide energy for training and help refill muscle energy stores5. For many active adults, about 1.4–2.0 g of protein per kilogram of body weight per day can support muscle growth when combined with resistance training2.
Muscle growth can be affected by smoking, heavy alcohol use, poor nutrition, not eating enough protein or calories, lack of regular strength training, and poor recovery14,15. Smoking is linked with lower muscle protein synthesis, while too much alcohol can slow muscle repair after exercise14.
Eating a protein-rich meal or snack every 3–4 hours can help support muscle protein synthesis throughout the day. After resistance exercise, eating high-quality protein soon after your workout may help muscles recover and grow over time2.
Two meals a day may make it harder for many people to meet their protein and energy needs for muscle gain. Spreading protein across several meals or snacks during the day may better support muscle repair and growth16.
Good snacks for muscle growth include low-fat yoghurt, fruit smoothies, bananas with a whey protein shake, and whole-grain cereal with milk. These snacks provide protein and carbohydrates, which help support muscle recovery and replenish energy after exercise5.
1. Ganson KT, Nguyen L, Ali ARH, et al. “Eat more protein, build more muscle”: A grounded theory study of muscle-building behaviors among Canadian adolescents and young adults. Body Image. 2023;47:101635. doi:10.1016/j.bodyim.2023.101635. Available from: https://pubmed.ncbi.nlm.nih.gov/37806066/
2. Jäger R, Kerksick CM, Campbell BI, et al. International Society of Sports Nutrition Position Stand: protein and exercise. J Int Soc Sports Nutr. 2017;14(1):20. doi:10.1186/s12970-017-0177-8. Available from: https://link.springer.com/article/10.1186/s12970-017-0177-8
3. Moore DR, Philp A. Editorial: Nutritional Strategies to Promote Muscle Mass and Function Across the Health Span. Front Nutr. 2020;7:569270. doi:10.3389/fnut.2020.569270. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7561707/
4. Iraki J, Fitschen P, Espinar S, Helms E. Nutrition Recommendations for Bodybuilders in the Off-Season: A Narrative Review. Sports. 2019;7(7):154. doi:10.3390/sports7070154. Available from: https://www.researchgate.net/publication/334044740_Nutrition_Recommendations_for_Bodybuilders_in_the_Off-Season_A_Narrative_Review
5. Hwang DJ, Yang HJ. Nutritional Strategies for Enhancing Performance and Training Adaptation in Weightlifters. Int J Mol Sci. 2024;26(1):240. doi:10.3390/ijms26010240. Available from: https://www.researchgate.net/publication/387572639_Nutritional_Strategies_for_Enhancing_Performance_and_Training_Adaptation_in_Weightlifters
6. ICMR–National Institute of Nutrition. Dietary Guidelines for Indians – 2024. Indian Council of Medical Research (ICMR), Department of Health Research, Ministry of Health and Family Welfare, Government of India; 2024. Accessed July 24, 2026. Available from: https://nin.res.in/dietaryguidelines/pdfjs/locale/DGI_2024.pdf
7. Strength training for beginners | healthdirect. Accessed July 24, 2026. Available from: https://www.healthdirect.gov.au/strength-training-for-beginners
8. Knowles OE, Drinkwater EJ, Urwin CS, Lamon S, Aisbett B. Inadequate sleep and muscle strength: Implications for resistance training. J Sci Med Sport. 2018;21(9):959-968. doi:10.1016/j.jsams.2018.01.012. Available from: https://europepmc.org/article/med/29422383
9. Exercise and Fluid Replacement. Med Sci Sports Exerc. 2007;39(2):377-390. doi:10.1249/mss.0b013e31802ca597. Available from: https://www.ovid.com/jnls/acsm-msse/abstract/10.1249/mss.0b013e31802ca597~exercise-and-fluid-replacement?redirectionsource=fulltextview
10. Helms ER, Aragon AA, Fitschen PJ. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. J Int Soc Sports Nutr. 2014;11(1):20. doi:10.1186/1550-2783-11-20. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4033492/
11. Rom O, Kaisari S, Aizenbud D, Reznick AZ. Lifestyle and Sarcopenia – Etiology, Prevention and Treatment. Rambam Maimonides Med J. 2012;3(4):e0024. doi:10.5041/RMMJ.10091. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3678825/
12. Centers for Disease Control and Prevention. How to Quit Smoking. May 2024. Available from: https://www.cdc.gov/tobacco/media/pdfs/2024/05/cdc-osh-how-to-quit-smoking-infographic-web-508.pdf
13. CDC. What You Can Do to Lower Your Risk of Alcohol-Related Harms. Alcohol Use. February 25, 2025. Accessed July 24, 2026. Available from: https://www.cdc.gov/alcohol/about-alcohol-use/lower-alcohol-related-harms.html
14. Parr EB, Camera DM, Areta JL, et al. Alcohol Ingestion Impairs Maximal Post-Exercise Rates of Myofibrillar Protein Synthesis following a Single Bout of Concurrent Training. Alway SE, ed. PLoS ONE. 2014;9(2):e88384. doi:10.1371/journal.pone.0088384. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0088384
15. Petersen AMW, Magkos F, Atherton P, et al. Smoking impairs muscle protein synthesis and increases the expression of myostatin and MAFbx in muscle. Am J Physiol-Endocrinol Metab. 2007;293(3):E843-E848. doi:10.1152/ajpendo.00301.2007. Available from: https://www.researchgate.net/publication/6229004_Smoking_impairs_muscle_protein_synthesis_and_increases_the_expression_of_myostatin_and_MAFbx_in_muscle
16. Schoenfeld BJ, Aragon AA. How much protein can the body use in a single meal for muscle-building? Implications for daily protein distribution. J Int Soc Sports Nutr. 2018;15(1):10. doi:10.1186/s12970-018-0215-1. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5828430/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Hearing your baby or child wake up in the middle of the night with a loud, barking cough can be frightening. This can often be a sign of croup cough, which is an inflammation of the windpipe. This blog will cover interesting facts, causes, symptoms, types, diagnosis, treatment, home remedies, and prevention of croup cough1.
Croup is an upper airway infection that is characterised by hoarseness and coughing that sounds like a seal barking. It is usually caused by viruses such as parainfluenza and RSV but can also be caused by bacteria. It is common in children under the age of 6. Most children with croup exhibit mild symptoms and can be treated at home, but in a few severe cases, hospitalisation is required1,2.
Croup is caused by viruses such as1,2:
Croup can also be caused by a bacterium, usually Staphylococcus aureus. In this case, it is called bacterial tracheitis.
The common types of croup that may occur in babies and kids include2:
Croup is diagnosed with the following examinations and laboratory tests1:
The options for croup treatment in babies and children include2:
Home remedies that may help soothe the symptoms of croup include3:
You may be able to avoid croup cough in your child by ensuring that they1,2:
Also Read: Home Remedies for Cold in Infants and Babies
It is important to consult a doctor if your child has croup and is not responding to any home remedies. If your child has trouble breathing, a high-pitched sound with every breath, extreme drowsiness, decreased consciousness, and bluish coloured lips and face, you should contact your doctor immediately3.
Also Read: Runny Nose in Children: Causes, How to Manage It & Prevention Tips
Although croup cases are usually mild and improve with care at home, some children may require hospitalisation. If your child develops breathing problems, extreme fatigue, and trouble swallowing, ensure that you go to the doctor as soon as possible. Recognising and diagnosing croup early, timely treatment, and appropriate care can help prevent complications. It is important to ensure hygiene and timely vaccinations for your child to avoid viral and bacterial infections in general.
If your child has a barking cough and hoarseness, it is likely that it is croup cough. Further tests, like a chest exam, may be needed to confirm the diagnosis1,3.
Yes, but it is important that you keep constantly checking with them at night. Make sure your child is not crying as it can worsen the symptoms. If your child is older than 1 year, it is advisable to use a pillow to keep their head up while sleeping1,3.
Antibiotics are administered to children only when a primary or secondary bacterial infection is suspected2.
Yes, the most severe symptoms of croup usually appear on day 3 or 42.
Sometimes, conditions such as acute epiglottitis (epiglottis infection), deep neck space abscesses (a condition characterised by fever, drooling, and neck stiffness), presence of a foreign body in the throat, and allergic reactions may be mistaken for croup as they all have similar symptoms2.
Yes, complications such as pneumonia may occur as a result of croup2.
1. Croup: MedlinePlus Medical Encyclopedia. Accessed July 3, 2026. Available from: https://medlineplus.gov/ency/article/000959.htm
2. Kadam S, Daley S, Carr B. Croup. StatPearls. Published online June 2, 2025. Accessed July 3, 2026. Available from: https://app-statpearls-legacy-prod.azurewebsites.net/point-of-care/20142
3. Croup – discharge: MedlinePlus Medical Encyclopedia. Accessed July 3, 2026. Available from: https://medlineplus.gov/ency/patientinstructions/000994.htm
4. Tracheitis: MedlinePlus Medical Encyclopedia. Accessed July 3, 2026. Available from: https://medlineplus.gov/ency/article/000988.htm
5. Content – Health Encyclopedia – URochester Medicine. Accessed July 16, 2026. Available from: https://www.urmc.rochester.edu/encyclopedia/content?contenttypeid=90&contentid=p02942
6. Treating Your Child’s “Barking Cough” at Home | University of Utah Health. January 2, 2023. Accessed July 16, 2026. Available from: https://healthcare.utah.edu/the-scope/kids-zone/all/2026/04/treating-your-childs-barking-cough-home
7. The-PEARL-No.-33_-Croup. Accessed July 20, 2026. Available from: https://flemsc.emergency.med.jax.ufl.edu/wordpress/files/2024/02/The-PEARL-No.-33_-Croup.pdf
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Many women experience changes such as irregular periods, sudden mood swings, persistent acne, or unexplained weight gain at some point in their lives. While these symptoms may often be dismissed as stress or part of a busy lifestyle, they may sometimes be linked to a hormonal imbalance1.
Hormones help regulate many body functions, and even small shifts in their levels can affect physical and emotional well-being2. In this article, we explain what hormonal imbalance in women means, the symptoms and causes to look out for, how it may be diagnosed and managed, and lifestyle measures that may support hormonal health.
Hormonal imbalance in women occurs when the body produces too much or too little of one or more hormones, or when hormone signals do not work as expected1,2. Hormones are chemical messengers made by glands such as the ovaries, thyroid, adrenal glands, and pituitary gland. They travel through the bloodstream and help regulate the menstrual cycle, fertility, metabolism, mood, sleep, and growth3.
Hormone levels naturally change during puberty, pregnancy, lactation, perimenopause, and menopause2. These changes are not always a cause for concern. However, when symptoms are persistent, severe, occur outside expected life stages, or interfere with daily life, they may point to a hormonal imbalance that needs medical evaluation. The type and severity of symptoms depend on which hormone is affected and the underlying cause.
Note: Hormonal imbalance is not a disease by itself; it is a sign that an underlying condition, life-stage change, medication, or lifestyle factor may be affecting normal hormone regulation.
Did You Know?
Hormonal imbalance can occur for many reasons. Some causes are a normal part of life, while others are linked to underlying medical conditions or lifestyle factors.
The symptoms of hormonal imbalance vary depending on which hormones are affected and the underlying cause. Some women experience only mild changes, while others may have symptoms that interfere with their daily lives. Common symptoms include1,12,15,17:
Your doctor will ask about your menstrual cycle, medical history, medications, lifestyle, and symptoms, and then perform a physical examination. Depending on your symptoms, your doctor may recommend one or more of the following tests:
Note: Hormone tests are not routinely recommended for every woman with suspected hormonal imbalance. Your doctor will order specific hormone tests based on your symptoms, medical history, physical examination, and suspected underlying condition.
Treatment for hormonal imbalance in women depends on the underlying cause, the hormones involved, your age, symptoms, and whether you are planning a pregnancy. In many cases, treating the underlying condition can help restore hormone balance and improve symptoms. Common management options include:
Note: Treatment focuses on identifying and managing the underlying cause of the hormonal imbalance rather than simply balancing hormones. So, the most appropriate treatment option depends on the specific condition causing the symptoms.
While lifestyle measures or home remedies for hormonal imbalance in women cannot treat the underlying cause, certain healthy habits can support overall hormonal health and help reduce symptoms. Some tips include:








Important: Home remedies and lifestyle changes may support hormonal health, but they cannot replace medical diagnosis or treatment when an underlying condition is present.
If not addressed, some hormonal imbalances can lead to long-term health problems. The risk and type of complications depend on the underlying cause and the hormones involved. Possible complications include1,5,22:

Although not all hormonal imbalances can be avoided, adopting healthy habits can help support normal hormone function and lower the risk of certain hormone-related conditions. Some tips include3,7,22:
Occasional hormonal fluctuations are normal, especially during puberty, pregnancy, lactation, perimenopause, and menopause. However, consult a doctor if symptoms are persistent, severe, worsening, or affecting your daily life. Seek medical advice if you have1,16,29,30:
Also Read: How to Store Insulin Safely During Travel: Tips, Precautions & Best Practices
Hormonal imbalance in women can affect menstrual cycles, fertility, mood, skin, weight, sleep, and metabolism. Some hormonal changes are a normal part of life, but symptoms that are persistent, severe, or disruptive should not be ignored because they may indicate an underlying medical condition.
Early evaluation, appropriate treatment, and healthy lifestyle habits can help manage symptoms and reduce the risk of complications. If you think you may have a hormonal imbalance, consult a doctor for an accurate diagnosis and a personalised treatment plan.
Hormonal imbalances can disrupt ovulation, the process in which the ovary releases a mature egg each month. This can make it more difficult to conceive naturally1,2.
This depends on the cause. Temporary hormonal changes, such as those during pregnancy or stress, may resolve on their own, while conditions like PCOS or thyroid disorders usually require ongoing management.
A doctor can evaluate your symptoms, review your medical history, perform a physical examination, and recommend tests such as blood tests, pelvic ultrasound, or other investigations to identify the underlying cause1,19,20.
Deficiencies of nutrients such as vitamin D and vitamin B12 may affect hormone production or function in some people31. However, hormonal imbalance is more commonly caused by medical conditions such as PCOS, thyroid disorders, or menopause1,2.
1. Almhmoud H, Alatassi L, Baddoura M, et al. Polycystic ovary syndrome and its multidimensional impacts on women’s mental health: A narrative review. Medicine (Baltimore). 2024;103(25):e38647. doi:10.1097/MD.0000000000038647. Available from: https://pubmed.ncbi.nlm.nih.gov/38905372/
2. Hiller-Sturmhöfel S, Bartke A. The Endocrine System. Alcohol Health Res World. 1998;22(3):153-164. Accessed July 21, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC6761896/
3. What Is a Hormone? National Institute of General Medical Sciences. Accessed July 21, 2026. https://nigms.nih.gov/biobeat/2024/07/what-is-a-hormone
4. Kolatorova L, Vitku J, Suchopar J, Hill M, Parizek A. Progesterone: A Steroid with Wide Range of Effects in Physiology as Well as Human Medicine. Int J Mol Sci. 2022;23(14):7989. doi:10.3390/ijms23147989. Available from: https://pubmed.ncbi.nlm.nih.gov/35887338/
5. Bartkowiak-Wieczorek J, Jaros A, Gajdzińska A, et al. The Dual Faces of Oestrogen: The Impact of Exogenous Oestrogen on the Physiological and Pathophysiological Functions of Tissues and Organs. Int J Mol Sci. 2024;25(15):8167. doi:10.3390/ijms25158167. Available from: https://pubmed.ncbi.nlm.nih.gov/39125736/
6. Moolhuijsen LME, Visser JA. Anti-Müllerian Hormone and Ovarian Reserve: Update on Assessing Ovarian Function. J Clin Endocrinol Metab. 2020;105(11):3361-3373. doi:10.1210/clinem/dgaa513. Available from: https://pubmed.ncbi.nlm.nih.gov/32770239/
7. Endocrine Disruptors. National Institute of Environmental Health Sciences. Accessed July 21, 2026. https://www.niehs.nih.gov/health/topics/agents/endocrine
8. Sender R, Kedar T, Navon Y, et al. The total mass, copy number, and distribution of hormones in the human bloodstream. PLOS Biol. 2026;24(6):e3003864. doi:10.1 371/journal.pbio.3003864. Available from: https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.3003864
9. Coussa A, Hasan HA, Barber TM. Impact of contraception and IVF hormones on metabolic, endocrine, and inflammatory status. J Assist Reprod Genet. 2020;37(6):1267-1272. doi:10.1007/s10815-020-01756-z. Available from: https://pubmed.ncbi.nlm.nih.gov/32215823/
10. Chen L, Lu Y, Zhou YF, et al. The effects of weight loss-related amenorrhea on women’s health and the therapeutic approaches: a narrative review. Ann Transl Med. 2023;11(2):132. doi:10.21037/atm-22-6366. Available from: https://pubmed.ncbi.nlm.nih.gov/36819572/
11. Valera H, Chen A, Grive KJ. The Hypothalamic-Pituitary-Ovarian Axis, Ovarian Disorders, and Brain Aging. Endocrinology. 2025;166(10):bqaf137. doi:10.1210/endocr/bqaf137. Available from: https://pubmed.ncbi.nlm.nih.gov/40884186/
12. Kaur J, Bhusal K. Hyperprolactinemia. StatPearls. November 30, 2025. Accessed July 23, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537331/
13. Kapoor E. Premature Ovarian Insufficiency. Curr Opin Endocr Metab Res. 2023;28:100435. doi:10.1016/j.coemr.2023.100435. https://pubmed.ncbi.nlm.nih.gov/36936056/
14. Saadedine M, Kapoor E, Shufelt C. Functional Hypothalamic Amenorrhea: Recognition and Management of a Challenging Diagnosis. Mayo Clin Proc. 2023;98(9):1376-1385. doi:10.1016/j.mayocp.2023.05.027. Available from: https://pubmed.ncbi.nlm.nih.gov/37661145/
15. Premenstrual syndrome (PMS). Women’s Health. Accessed July 21, 2026. https://womenshealth.gov/menstrual-cycle/premenstrual-syndrome
16. Santoro N, Epperson CN, Mathews SB. Menopausal Symptoms and Their Management. Endocrinol Metab Clin North Am. 2015;44(3):497-515. doi:10.1016/j.ecl.2015.05.001. Available from: https://pubmed.ncbi.nlm.nih.gov/26316239/
17. Tarney CM, Han J. Postcoital Bleeding: A Review on Etiology, Diagnosis, and Management. Obstet Gynecol Int. 2014;2014:192087. doi:10.1155/2014/192087. Available from: https://pubmed.ncbi.nlm.nih.gov/25045355/
18. Dreisler E, Frandsen CS, Ulrich L. Perimenopausal abnormal uterine bleeding. Maturitas. 2024;184:107944. doi:10.1016/j.maturitas.2024.107944. Available from: https://pubmed.ncbi.nlm.nih.gov/38412750/
19. Hormone levels: MedlinePlus. Accessed July 21, 2026. https://medlineplus.gov/ency/article/003445.htm
20. Wang F, Liu J, Zhang R, et al. CT and MRI of adrenal gland pathologies. Quant Imaging Med Surg. 2018;8(8):853-875. doi:10.21037/qims.2018.09.13. Available from: https://pubmed.ncbi.nlm.nih.gov/30306064/
21. Healthy diet. World Health Organization. Accessed July 21, 2026. https://www.who.int/news-room/fact-sheets/detail/healthy-diet
22. Teede HJ, Tay CT, Laven JJE, et al. Recommendations From the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2023;108(10):2447-2469. doi:10.1210/clinem/dgad463. Available from: https://pubmed.ncbi.nlm.nih.gov/37580314/
23. Khajuria A, Kumar A, Joshi D, Kumaran SS. Reducing Stress with Yoga: A Systematic Review Based on Multimodal Biosignals. Int J Yoga. 2023;16(3):156-170. doi:10.4103/ijoy.ijoy_218_23. Available from: https://pubmed.ncbi.nlm.nih.gov/38463652/
24. Direksunthorn T. Sleep and Cardiometabolic Health: A Narrative Review of Epidemiological Evidence, Mechanisms, and Interventions. Int J Gen Med. 2025;18:5831-5843. doi:10.2147/IJGM.S563616. Available from: https://pubmed.ncbi.nlm.nih.gov/41035532/
25. Rachdaoui N, Sarkar DK. Effects of alcohol on the endocrine system. Endocrinol Metab Clin North Am. 2013;42(3):593-615. doi:10.1016/j.ecl.2013.05.008. Available from: https://pubmed.ncbi.nlm.nih.gov/24011889/
26. Tweed JO, Hsia SH, Lutfy K, Friedman TC. The endocrine effects of nicotine and cigarette smoke. Trends Endocrinol Metab. 2012;23(7):334-342. doi:10.1016/j.tem.2012.03.006. Available from: https://pubmed.ncbi.nlm.nih.gov/22561025/
27. Office of Dietary Supplements. Omega-3 Fatty Acids. Accessed July 21, 2026. https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/
28. Office of Dietary Supplements. Vitamin D. Accessed July 21, 2026. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
29. Mazzarello S, Arnaout A. Nipple discharge. CMAJ Can Med Assoc J. 2015;187(8):599. doi:10.1503/cmaj.140633. Available from: https://pubmed.ncbi.nlm.nih.gov/25733736/
30. Unnikrishnan AG, Menon UV. Thyroid disorders in India: An epidemiological perspective. Indian J Endocrinol Metab. 2011;15(Suppl2):S78-S81. doi:10.4103/2230-8210.83329. Available from: https://pubmed.ncbi.nlm.nih.gov/21966658/
31. Aktaş HŞ. Vitamin B12 and Vitamin D Levels in Patients with Autoimmune Hypothyroidism and Their Correlation with Anti-Thyroid Peroxidase Antibodies. Med Princ Pract. 2020;29(4):364-370. doi:10.1159/000505094. Available from: https://pubmed.ncbi.nlm.nih.gov/31779003/
32. Ranabir S, Reetu K. Stress and hormones. Indian J Endocrinol Metab. 2011;15(1):18-22. doi:10.4103/2230-8210.77573. Available from: https://pubmed.ncbi.nlm.nih.gov/21584161/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
Headaches are among the most common health conditions, affecting individuals of all ages across the world. According to the World Health Organisation (WHO), headache disorders affect over 40% of the world’s population1. While many people have occasional headaches, regular episodes can interfere with work, sleep, and other everyday activities. Understanding the different types of headaches can help identify their causes and improve their treatment and prevention2. In this blog, we will discuss how many types of headaches are there, their causes, how they are diagnosed, their treatment options, and simple tips to prevent them.
A headache is a pain or discomfort felt in the head, scalp, or face. It can range from mild to severe and may last for a few minutes or several hours2. Headaches occur when pain-sensitive structures in and around the head, such as blood vessels, nerves, muscles, and tissues, become irritated or triggered due to factors such as smell, stress, and medications2,3.
Headaches, especially when they occur frequently, can affect a person’s quality of life and even cause problems at work. The fear of getting another headache can greatly affect family relationships, social activities, and job performance. Living with long-term headaches may also increase the risk of other health problems, such as anxiety and depression, which is more commonly observed in people with migraines, a type of headache1.
There are two types of headaches: primary headaches and secondary headaches. The table below highlights the key differences between these two types:
| Feature | Primary Headaches | Secondary Headaches |
| Definition | Headaches that are not caused by any medical condition, but are a part of a headache disorder4. | Headaches that occur due to an underlying health problem5. |
| Common causes | Occurs due to complex changes in the brain and nervous system mechanisms that are involved in sensing and processing pain4. Factors such as stress, hormonal changes, lack of sleep, certain foods, and genetics can act as a trigger that brings on headache episodes2. | Occurs when an underlying health condition irritates or puts pressure on the pain-sensitive structures in the head and neck (such as nerves, brain covering [meninges], blood vessels, muscles and tissues covering the skull). These conditions can include brain infections, head injuries, medication overuse, extremely high blood pressure, acute sinus infections (long-term infections rarely cause headaches), strokes, tumours, and other brain disorders2,5. |
| Examples | Migraine, tension headache, cluster headache, etc.4. | Sinus headache, medication-overuse headache, cervicogenic headache, etc5. |
| Severity | Usually not life-threatening, but can interfere with quality of life1,4. | Depends on the cause and can range from mild to life-threatening5. |
| Treatment | Symptom management, trigger avoidance and prescription medications if needed2. | Treating underlying health condition5. |
Understanding the different types of headaches and their causes can help you identify possible triggers, recognise warning signs, and seek the right treatment when needed. Here are some of the common types of headaches:

These are among the most common types of primary headaches. They usually last between 30 minutes and one week. Although they can start around puberty, they are most common in people in their 30s. Women and young people are more likely to experience this headache.

This is a type of primary headache that occurs repeatedly2. It can last between 4 and 72 hours. It often begins during puberty and is most common in people aged 35 to 45 years. Women are more likely to be affected than men due to hormonal issues. Migraine attacks in children are usually shorter than in adults1.
Note: Food triggers can vary from person to person. Alcohol (especially red wine), excess caffeine intake or suddenly stopping caffeine, chocolate, fish, and processed meats may trigger migraines in some people.
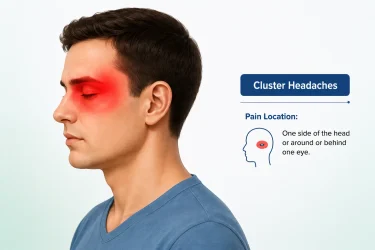
These are extremely painful but rare types of primary headaches. They can last from 15 minutes to 3 hours. The pain occurs in clusters or as repeated episodes, at the same time each day or night for many weeks. They most commonly occur between the ages of 20 and 40 years but can occur at any age, including in children and older adults2. These are more common in men than in women7.
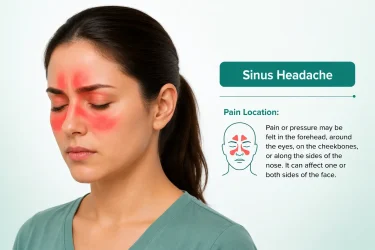
This is a type of secondary headache caused by the sinus issues9. Without treatment, the pain can persist for 4 weeks or less than that and become worse when a person bends forward or lies down. However, in most cases, the headache usually improves as the infection subsides9,10.
Note: Many headaches that people believe are caused by sinus problems are actually migraines. This is a common misunderstanding about headaches7.

This is a type of secondary headache, which is rare and chronic. It is most commonly seen in people aged between 30 and 44 years. It is often mistaken for primary headaches, such as migraine and tension-type headache. The pain goes away when the underlying condition is treated successfully.

This is a type of secondary headache caused by the overuse of medications. It is also known as rebound headache. Medication-overuse headache is characterised as:
As there are different types of headaches and their reasons vary, doctors might use more than one diagnostic procedure to determine the cause of a headache. These include:
Note: High BP causes headache only when it causes hypertensive emergencies or BP rises suddenly. Mild or moderate high blood pressure does not usually cause headaches.
Note: If the doctor suspects that the increased pressure inside the skull is caused by a tumour or another growth, they may recommend a CT scan or MRI before considering a lumbar puncture. In some cases, a lumbar puncture may not be safe.
The treatment options usually available for headaches include:
Frequent headaches can often be managed by identifying and avoiding the triggers that cause them. The following measures may help lower the risk of recurrent headaches:





Also Read: Home Remedies For Headache By Dr. Siddharth Gupta
It is very important to consult a doctor if the headache:
Headaches are a common ailment and their severity can range from a mild ache to severe pain that interferes with daily activities. While most headaches are harmless, some may be a sign of an underlying health problem that needs medical attention. Knowing the different types of headaches, their symptoms, causes, and treatments can help you manage them better and recognise when to see a doctor.
The 5 C’s of headaches are common triggers that can worsen or cause headaches: Cheese, chocolate, citrus fruits, caffeine, and coke. Avoiding these triggers may help reduce headaches in some people, especially those with migraines16.
The type of headache can often be identified by its location, how the pain feels, how long it lasts, and its symptoms (such as nausea, sensitivity to light, or nasal congestion). A doctor might correlate these along with the individual’s medical history and triggers and, in some cases, recommend tests to rule out serious underlying conditions2,10.
Headaches that start suddenly and are severe; occur after a head injury; or are accompanied by symptoms such as weakness, confusion, seizures, fever, vision changes, or difficulty speaking require immediate medical attention as they may be a sign of serious conditions such as a stroke, meningitis, or bleeding in the brain2,5.
Consult a doctor immediately if your headaches are sudden or severe, occur after a head injury, or are associated with fever, confusion, weakness, vision problems, seizures, or difficulty speaking. These symptoms may be a sign of a serious condition and should not be ignored2.
A brain tumour-related headache is usually persistent, gradually worsens over time, and may be worse in the morning or with coughing and straining. It is important to note that these symptoms may also occur if a person has a migraine or cluster headache. A person with tumour may have other associated symptoms, such as seizures, vision changes, weakness, or difficulty speaking. Most headaches are not caused by brain tumours; however, a new or worsening headache with neurological symptoms should be evaluated by a doctor5.
1. Migraine and other headache disorders. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/headache-disorders
2. Headache. 2026. Available from: https://www.ninds.nih.gov/health-information/disorders/headache
3. The anatomy of head pain. In: Handbook of Clinical Neurology. Vol 198. Elsevier; 2023:41-60. doi:10.1016/B978-0-12-823356-6.00001-9 Available from: https://pubmed.ncbi.nlm.nih.gov/38043970/
4. Wang Z, Yang X, Zhao B, Li W. Primary headache disorders: From pathophysiology to neurostimulation therapies. Heliyon. 2023;9(4):e14786. doi:10.1016/j.heliyon.2023.e14786 Available from: https://pubmed.ncbi.nlm.nih.gov/37077680/
5. Wijeratne T, Wijeratne C, Korajkic N, Bird S, Sales C, Riederer F. Secondary headaches – red and green flags and their significance for diagnostics. eNeurologicalSci. 2023;32:100473. doi:10.1016/j.ensci.2023. 100473 Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10339125/
6. Nihir Shah, Asuncion RMD, Hameed S. Muscle Contraction Tension Headache. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562274/
7. Headache: When to worry, what to do. 2024. Available from: https://www.health.harvard.edu/pain/headache-when-to-worry-what-to-do
8. Cluster headache. 2025. Available from: https://medlineplus.gov/ency/article/000786.htm
9. Sinusitis. 2024. Available from: https://medlineplus.gov/ency/article/000647.htm
10. Headaches. 2025. Available from: https://www.healthdirect.gov.au/headaches
11. Al Khalili Y, K. Ly N, Murphy PB. Cervicogenic Headache. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507862/
12. Aleksenko D, Lui F, Sánchez-Manso JC. Medication Overuse Headache. 2025. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK470171/
13. Medication Overuse Headache. 2022. Available from: https://headaches.org/resources/medication-overuse-headache/
14. Kim KT. Lumbar puncture: considerations, procedure, and complications. encephalitis. 2022;2(4):93-97. doi:10.47936/encephalitis.2022.00045 Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10295920/
15. Eskey CJ, Ogilvy CS. Fluoroscopy-guided lumbar puncture: decreased frequency of traumatic tap and implications for the assessment of CT-negative acute subarachnoid hemorrhage. AJNR Am J Neuroradiol. 2001;22(3):571-576. Available from: https://pubmed.ncbi.nlm.nih.gov/11237986/
16. Speight N. Best practice: migraine. Arch Dis Child. 2006 Jun;91(6):541. PMID: 16714736; PMCID: PMC2082764. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2082764/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.

Kidney disease often develops quietly, with little or no warning in its early stages. That is why many individuals do not realise there is a problem until the condition has progressed to an advanced stage1.
However, recognising the early signs of kidney disease and seeking timely medical care can help slow or even avoid further kidney damage.
In this blog, we will explore the early kidney disease symptoms, types and causes, lifestyle and prevention tips, and when it is important to consult a doctor.
Healthy kidneys filter waste products, excess fluid, and toxins from the blood. They also help regulate blood pressure, maintain the body’s fluid and mineral balance, and produce hormones that support bone health and red blood cell production2. Kidney disease occurs when the structure or function of the kidney is impaired. This can cause waste and fluid to build up in the body3,4.
Did You Know?
Depending on the rate at which the symptoms have developed, kidney disease can be of two main types4:
The seriousness of your kidney disease is primarily determined by your eGFR (estimated glomerular filtration rate), which measures how effectively your kidneys filter waste from your blood, and your uACR (urine albumin-to-creatinine ratio), which assesses kidney damage and protein leakage.

AKI develops suddenly over hours or days. A sudden drop in kidney function, suggesting AKI, would typically be associated with one or more of the following kidney disease symptoms6:
Important: AKI is a medical emergency and requires prompt evaluation and treatment. Early intervention can often restore kidney function and help avoid long-term damage4,6.
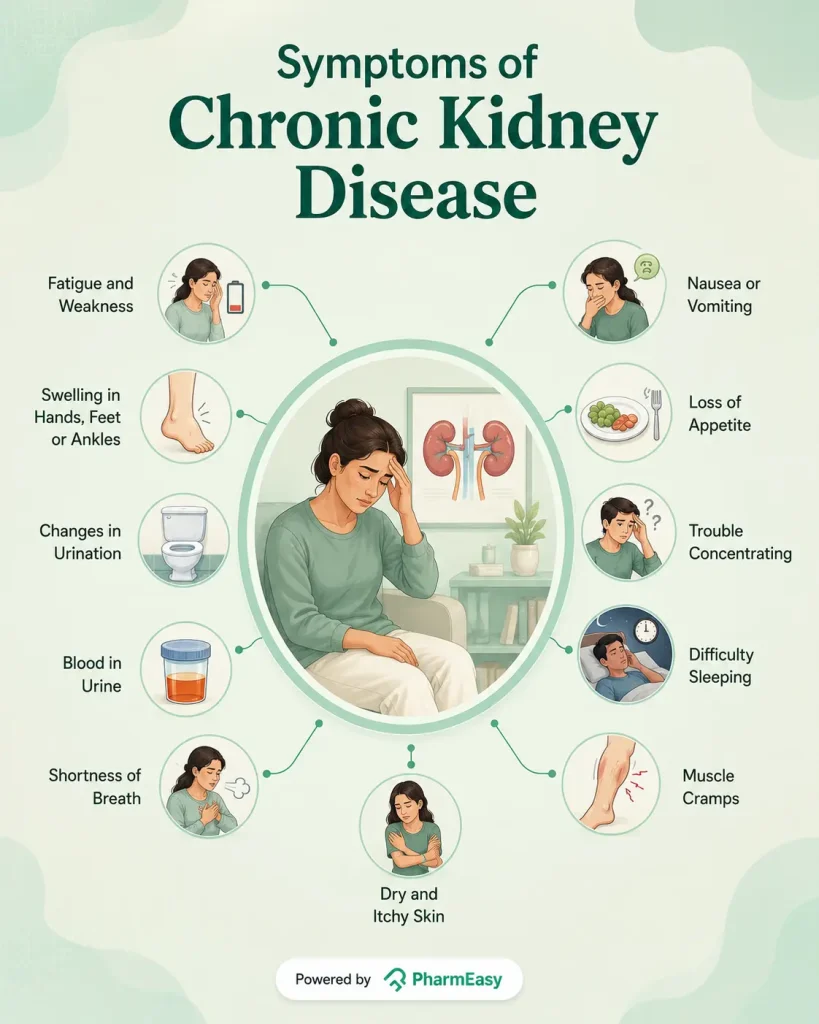
Some early signs and symptoms of CKD include:
Note: Many individuals with early CKD have no symptoms at all. Kidney disease is often detected during routine blood or urine tests performed for conditions such as diabetes or high blood pressure10.
The causes of kidney disease depend on whether it develops suddenly (AKI) or gradually (CKD).
AKI occurs when the kidneys suddenly stop working properly, often due to an illness, injury, or reduced blood flow to the kidneys. Common causes include6:
Note: The iodinated contrast dye used in some imaging tests, such as CT scans and angiography, may increase the risk of AKI in individuals with existing kidney disease or other risk factors. However, for most individuals with healthy kidneys, the risk is low6,11.
CKD develops gradually and is usually caused by long-term conditions that damage the kidneys over time. Common causes include12:
Recognising signs of kidney disease early can make a substantial difference in protecting your kidney health and overall well-being. Early detection is important for several reasons1,13:
If your doctor suspects kidney disease, they may recommend one or more of the following tests to assess how well your kidneys are working and identify the underlying cause6,14:
Note: In cases of AKI, doctors may also monitor urine output closely and perform additional tests, such as an ECG or imaging studies, depending on the suspected cause.
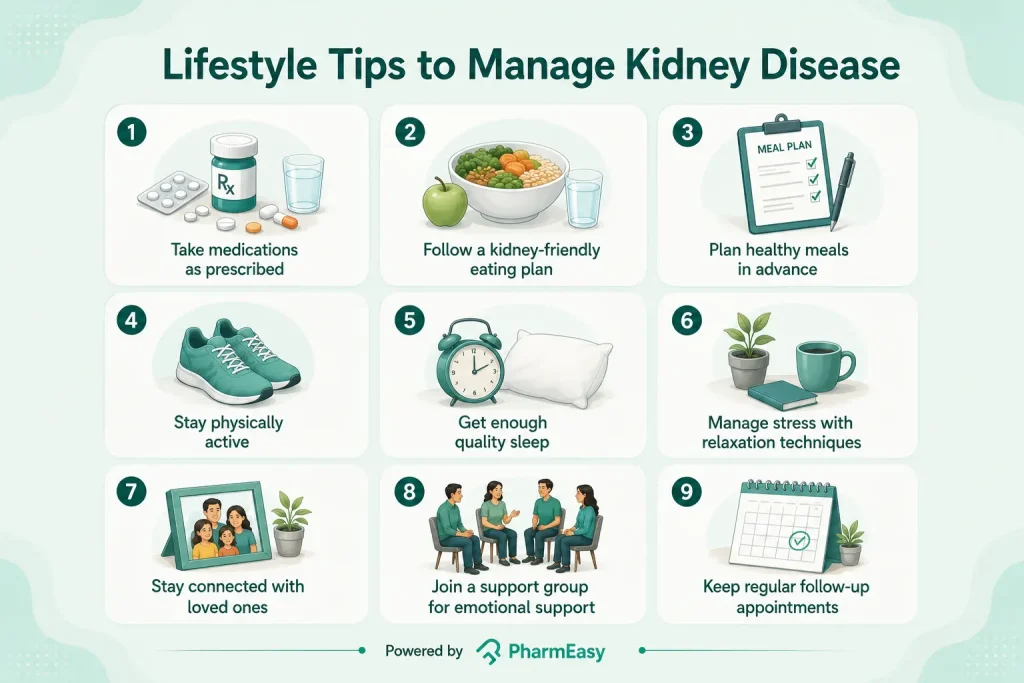
Living with kidney disease involves more than taking medications. There are several lifestyle habits that you can follow to slow disease progression, improve your quality of life, and support your overall well-being:
Also Read: Diet Chart for Kidney Patients Along with Helpful Tips
While not all kidney diseases can be prevented, healthy lifestyle habits can significantly reduce your risk. Prevention is especially important if you have diabetes, high blood pressure, heart disease, or a family history of kidney disease. Some tips for preventing kidney disease include16:
Note: Excessive water intake does not prevent CKD and can even be harmful for individuals who have been advised to restrict their fluid intake.
Also Read: High Uric Acid Level: Causes, Risks, Treatment, Prevention
Do not ignore persistent symptoms of kidney disease that could indicate a kidney problem. Early medical attention can help identify kidney disease before it becomes more serious. Consult a doctor if you6,10:
Also Read: High Creatinine: Symptoms, Causes, Diagnosis & Treatment
Kidney disease is a common but often overlooked condition that can have serious health consequences if left untreated. Therefore, knowing the early signs of kidney disease and understanding your risk can help you act before significant kidney damage occurs.
Remember, with timely medical care and healthy lifestyle choices, it is possible to protect your kidney function and maintain your overall health for years to come.
CKD is divided into five stages based on the eGFR and UACR, which measure how well the kidneys are filtering blood. Stage 1 involves mild kidney damage with normal kidney function, Stage 2 is characterised by mild to moderate loss of kidney function, Stage 3 involves moderate loss of kidney function, Stage 4 indicates severe loss of kidney function, and Stage 5 indicates kidney failure13.
Advanced kidney disease can cause unintended weight loss due to poor appetite, nausea, vomiting, and the buildup of waste products in the body. However, some individuals may initially gain weight because of fluid retention10,17.
If left untreated, kidney disease can lead to kidney failure and increase the risk of serious complications, including high blood pressure, heart disease, anaemia, and bone disorders3. Therefore, early diagnosis and management are important to help slow disease progression and reduce these risks.
1. Whaley-Connell A, Nistala R, Chaudhary K. The Importance of Early Identification of Chronic Kidney Disease. Mo Med. 2011;108(1):25-28. https://pubmed.ncbi.nlm.nih.gov/21462606/
2. Your Kidneys & How They Work – NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. Accessed July 3, 2026. https://www.niddk.nih.gov/health-information/kidney-disease/kidneys-how-they-work
3. Vaidya SR, Aeddula NR. Chronic Kidney Disease. In: StatPearls. StatPearls Publishing; 2026. Accessed July 3, 2026. http://www.ncbi.nlm.nih.gov/books/NBK535404/
4. Kidney disease. Accessed July 3, 2026. https://www.who.int/news-room/fact-sheets/detail/kidney-disease
5. Global Facts: About Kidney Disease | National Kidney Foundation. Accessed July 3, 2026. https://www.kidney.org/global-facts-about-kidney-disease
6. Acute kidney injury (AKI). nhs.uk. October 3, 2018. Accessed July 3, 2026. https://www.nhs.uk/conditions/acute-kidney-injury/
7. Khitan ZJ, Glassock RJ. Foamy Urine. Clin J Am Soc Nephrol CJASN. 2019;14(11):1664-1666. doi:10.2215/CJN.06840619 https://pubmed.ncbi.nlm.nih.gov/31575619/
8. 10 Signs You May Have Kidney Disease | National Kidney Foundation. Accessed July 3, 2026. https://www.kidney.org/news-stories/10-signs-you-may-have-kidney-disease
9. Hematuria (Blood in the Urine) – NIDDK. Accessed July 6, 2026. https://www.niddk.nih.gov/health-information/urologic-diseases/hematuria-blood-urine
10. Chronic kidney disease – Symptoms. nhs.uk. October 3, 2018. Accessed July 3, 2026. https://www.nhs.uk/conditions/kidney-disease/symptoms/
11. Wang KC, Lin LC, Pan SY, et al. Use of iodinated and gadolinium-based contrast media in patients with chronic kidney disease: Consensus statements from nephrologists, cardiologists, and radiologists at National Taiwan University Hospital. J Formos Med Assoc. 2026;125(3):261-267. doi:10.1016/j.jfma.2025.01.019 https://pubmed.ncbi.nlm.nih.gov/39870554/
12. Chronic kidney disease. nhs.uk. October 20, 2017. Accessed July 3, 2026. https://www.nhs.uk/conditions/kidney-disease/
13. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease – PubMed. Accessed July 3, 2026. https://pubmed.ncbi.nlm.nih.gov/38490803/
14. Chronic kidney disease – Diagnosis. nhs.uk. October 20, 2017. Accessed July 3, 2026. https://www.nhs.uk/conditions/kidney-disease/diagnosis/
15. 8 Self-Care Ideas for People With Chronic Kidney Disease (CKD) | National Kidney Foundation. Accessed July 3, 2026. https://www.kidney.org/news-stories/8-self-care-ideas-people-kidney-disease
16. Preventing Chronic Kidney Disease – NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. Accessed July 3, 2026. https://www.niddk.nih.gov/health-information/kidney-disease/chronic-kidney-disease-ckd/prevention
17. Singer R, Huang H. Weight change in chronic kidney disease: Association with mortality and kidney function. Obes Sci Pract. 2023;10(1):e723. doi:10.1002/osp4.723 https://pubmed.ncbi.nlm.nih.gov/38264010/
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.
7
A headache is a common problem that makes it difficult to study, work, or enjoy any activities you do. Although headaches may not be severe in most cases, sometimes they may be a cause for concern. However, knowing their cause can help you get the right treatment you need1. In this blog, we’ll cover the common causes and symptoms of headaches, the available treatment options, and simple ways to help manage them.
A headache is a pain or discomfort arising from pain-sensitive structures in the head, such as the blood vessels, nerves, and the tissues covering the brain (meninges)2. This pain occurs because of changes in the way the brain, nerves, and blood vessels process pain signals. It can occur in different parts of the head, scalp, or face. It may feel dull, sharp, throbbing, or like a tight band wrapped around the head. Headaches can last from a few minutes to several hours or, in some cases, even days, depending on the underlying cause. While most headaches are not serious and improve with simple treatment, some may be a sign of an underlying health condition that requires medical attention1.
Did You Know?
Headaches are broadly classified into primary headaches and secondary headaches, depending on whether the headache itself is the main condition or is caused by another medical problem.
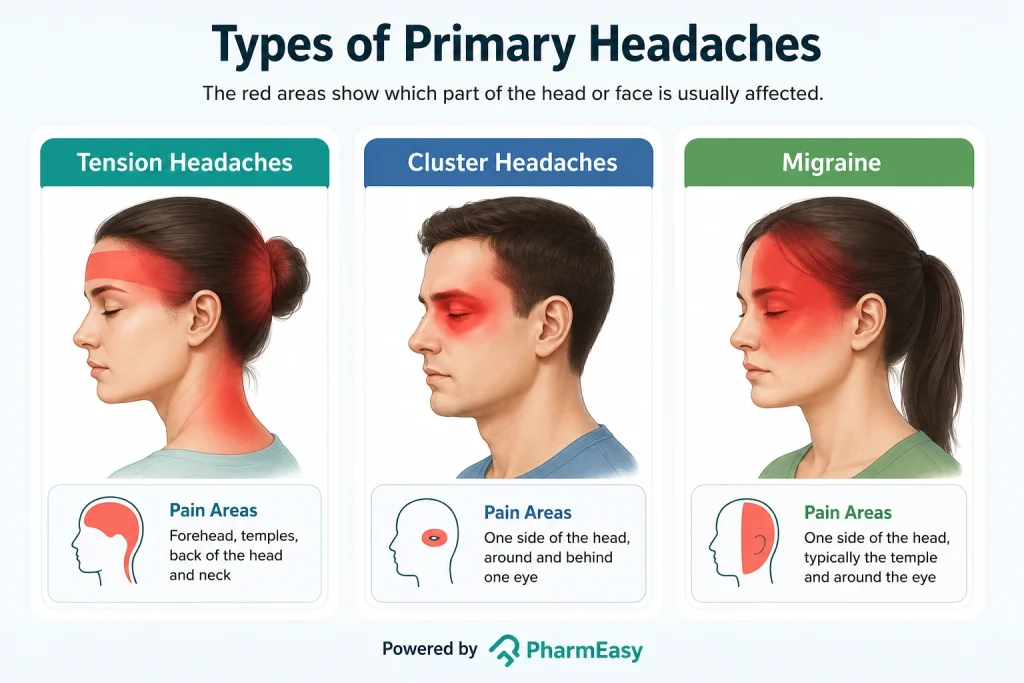
Headaches that occur because of changes in the pain-sensitive structures of the head or the way the brain processes pain are called primary headaches. They may not be caused by an underlying health condition. The different types of headaches (primary) include:
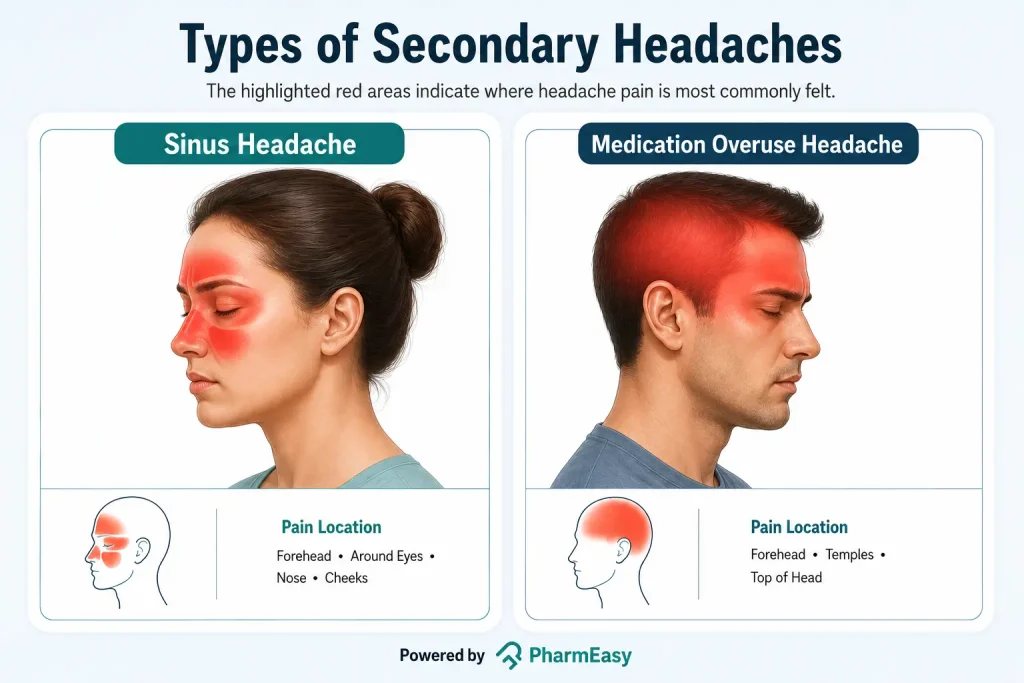
This is a type which indicates an underlying health condition, such as high blood pressure (BP), infection, or head injury. It can last from a few minutes to several days, weeks, or even months, depending on the underlying cause8. It happens when the condition affects the pain-sensitive tissues or nerves in the head. It is less common, but needs prompt medical evaluation and treatment for the underlying cause rather than the headache itself1. Examples include:
Other types of secondary headaches include post-traumatic headache (related to head injury or trauma), headaches related to an arterial ischemic event (caused by reduced blood flow to the brain due to a stroke), headaches related to arthritis, hypertension headache (caused by extremely high BP), and reversible cerebral vasoconstriction syndrome (caused by temporary narrowing of the blood vessels in the brain)8.
Headache symptoms can vary based on the type. While some symptoms are specific to certain types of headaches, there are a few common signs and symptoms that many people with headaches may experience. These include:
The causes of headaches vary depending on the type. Some of the most common headache causes include the following.
In addition to understanding the causes of headaches, knowing the risk factors is very important to reduce the risk or manage the condition. Factors that may increase the risk of a person having headaches include:
Note: These are common risk factors for many types of headaches. Having one or more of these risk factors does not guarantee you’ll get headaches.
The following are the approaches a doctor might take to identify the type of headache:
Headache treatment is determined by its type, severity, frequency, and underlying reason. While some headaches can be treated with simple lifestyle adjustments, others may necessitate prescription medications or therapy for the underlying medical issue. The treatment approaches that are commonly recommended include:
Depending on the type of headache, the doctor may recommend pain-relieving medicines, such as paracetamol or ibuprofen16, triptans or beta-blocker medicines (for migraine), antidepressants or barbiturates (for tension headaches; barbiturates are not routinely recommended due to a risk of medication overuse headache), verapamil (for cluster headaches)1. Although some of these medicines are available as over-the-counter medicines, taking them too often or without a doctor’s advice is not advisable12.
Headaches caused by an underlying medical condition (secondary headaches), such as sinus infections, high BP, or brain tumours, require treatment of the underlying cause. This may include antibiotics, nasal corticosteroid sprays or anti-histamines (for sinus infection)10, BP medications (for high BP), surgery (for tumours), etc.8, depending on the cause.
Exercises, stretching, and posture correction to help with tension headaches or headaches caused by muscle strain4.
Surgeries, chemotherapy, etc., in cases where the headaches do not respond to medicines, for example, a tumour that is causing a headaches5.
Note: Headache treatment differs from person to person based on the type, severity, frequency, and underlying cause. Do not self-medicate or take pain relievers on a regular basis without consulting a doctor, since this can worsen headaches.
People often wonder how to reduce headaches naturally. The best approach is to prevent headaches rather than treating them after they occur. Here are some simple ways to help reduce the risk of getting a headache:

Identifying and avoiding personal headache triggers, such as certain foods, alcohol, smoking, dehydration, bright lights, lack of sleep, improper posture, etc., can help reduce headache episodes.

Deep breathing, meditation, yoga, regular exercise and other relaxation methods can help reduce stress-related headaches1.

Undergoing regular health check-ups, especially in people with conditions such as high BP or allergies, can help identify and manage factors that may contribute to headaches.
Note: These recommendations may help reduce the frequency or severity of headaches, but they do not guarantee perfect prevention. If headaches are severe, frequent, sudden, or persistent despite these precautions, see a doctor for a correct diagnosis and treatment.
Also Read: Home Remedies For Headache By Dr. Siddharth Gupta
Consult a doctor if:
Headaches are common and, in most cases, do not indicate a major health problem. They might be caused by common conditions like stress, dehydration, lack of sleep, or illness, but they can also be symptoms of an underlying medical disease. Consult a doctor immediately for an accurate diagnosis and treatment if headaches are severe, frequent, or accompanied by strange symptoms. Understanding the various types, symptoms, and triggers might help in managing headaches more successfully.
Morning headaches can be caused by poor sleep, dehydration (mainly from alcohol consumption), stress, teeth grinding, sleep apnoea (interrupted breathing during sleep), and excessive medication use. In such cases, it is important to see a doctor to determine the underlying reason and get the right treatment17.
Headaches that worsen while bending down are commonly caused by sinus congestion or a sinus infection, as bending increases pressure in the inflamed sinuses6. However, it is important to consult a doctor for a proper diagnosis and treatment, as headaches when bending down can also be caused by other underlying conditions17.
Yes, skipped meals, especially breakfast, can result in headaches. Going too long without eating can cause blood sugar levels to drop, causing a headache, particularly in people who are prone to migraines6,17.
Yes. Dehydration may cause headaches by lowering the amount of fluid in the body,1,6 which disrupts proper brain function. Drinking plenty of water throughout the day can help avoid dehydration-related headaches. Dehydration may also occur from excessive drinking of alcohol, thereby contributing to headache17.
Yes. Lack of sleep can cause headaches by altering how your brain responds to pain. Maintaining a regular sleep schedule and getting enough rest can help lower the risk of headaches.
Headaches can happen for many reasons, including stress, lack of sleep, dehydration, skipping meals, eye strain, infections, or underlying medical conditions. Identifying the cause can help in choosing the right treatment1.
Taking a painkiller for a headache too often can actually cause more frequent headaches (medication overuse headaches). You should consult a doctor if you have recurring headaches to identify the cause rather than taking an over-the-counter medication1,12.
The best way to treat a headache depends on its cause. Resting, staying hydrated, eating a light meal if it is skipped, and taking pain-relieving medicines, if advised by a doctor or avoiding them in case of medication-overdose headaches, etc., can help relieve most common headaches1,12.
1. Headache. 2026. Available from: https://www.ninds.nih.gov/health-information/disorders/headache
2. Robertson CE, Benarroch EE. The anatomy of head pain. Handb Clin Neurol. 2023;198:41-60. doi: 10.1016/B978-0-12-823356-6.00001-9. PMID: 38043970. Available from: https://pubmed.ncbi.nlm.nih.gov/38043970/
3. Migraine and other headache disorders. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/headache-disorders
4. Nihir Shah, Asuncion RMD, Hameed S. Muscle Contraction Tension Headache. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562274/
5. The Complete Headache Chart. Available from: https://headaches.org/resources/the-complete-headache-chart/
6. Headaches. 2025. Available from: https://www.healthdirect.gov.au/headaches
7. Joppeková Ľ, Pinto MJ, Da Costa MD, et al. What does a migraine aura look like?—A systematic review. J Headache Pain. 2025;26(1):149. doi:10.1186/s10194-025-02080-6 Available from: https://pubmed.ncbi.nlm.nih.gov/40597581/
8. Wijeratne T, Wijeratne C, Korajkic N, Bird S, Sales C, Riederer F. Secondary headaches – red and green flags and their significance for diagnostics. eNeurologicalSci. 2023 Jun 30;32:100473. doi: 10.1016/j.ensci.2023.100473. PMID: 37456555; PMCID: PMC10339125. Available from: https://pubmed.ncbi.nlm.nih.gov/37456555/
9. Jones NS. Sinus headaches: avoiding over- and mis-diagnosis. Expert Review of Neurotherapeutics. 2009;9(4):439-444. doi:10.1586/ern.09.8 Available from: https://pubmed.ncbi.nlm.nih.gov/19344297/
10. Sinusitis. 2024. Available from: https://medlineplus.gov/ency/article/000647.htm
11. How to Know if You Have Migraine or Sinus Headache. 2023. Available from: https://americanmigrainefoundation.org/resource-library/sinus-headache/
12. Medication Overuse Headache. 2022. Available from: https://headaches.org/resources/medication-overuse-headache/
13. Aggarwal M, Puri V, Puri S. Serotonin and CGRP in migraine. Ann Neurosci. 2012 Apr;19(2):88-94. doi: 10.5214/ans.0972.7531.12190210. PMID: 25205974; PMCID: PMC4117050. Available from: https://pubmed.ncbi.nlm.nih.gov/25205974/
14. Sinus Infection Basics. 2024. Available from: https://www.cdc.gov/sinus-infection/about/index.html
15. Kim KT. Lumbar puncture: considerations, procedure, and complications. encephalitis. 2022;2(4):93-97. doi:10.47936/encephalitis.2022.00045 Available from: https://pubmed.ncbi.nlm.nih.gov/37469996/
16. Medicines for headaches. 2025. Available from: https://www.healthdirect.gov.au/medicines-for-headaches
17. Hong Y, Kang MK, Kim MS, Mo H, Cox RC, Im HJ. Morning Headaches: An In-depth Review of Causes, Associated Disorders, and Management Strategies. Headache and Pain Research. 2025;26(1):66-79. doi:10.62087/hpr.2024.0023 Available from: https://www.researchgate.net/publication/405443332_Comments_on_Morning_Headaches_An_In-Depth_Review_of_Causes_Associated_Disorders_and_Management_Strategies
Disclaimer: The information provided here is for educational/awareness purposes only and is not intended to be a substitute for medical treatment by a healthcare professional and should not be relied upon to diagnose or treat any medical condition. The reader should consult a registered medical practitioner to determine the appropriateness of the information and before consuming any medication. PharmEasy does not provide any guarantee or warranty (express or implied) regarding the accuracy, adequacy, completeness, legality, reliability or usefulness of the information; and disclaims any liability arising thereof.
Links and product recommendations in the information provided here are advertisements of third-party products available on the website. PharmEasy does not make any representation on the accuracy or suitability of such products/services. Advertisements do not influence the editorial decisions or content. The information in this blog is subject to change without notice. The authors and administrators reserve the right to modify, add, or remove content without notification. It is your responsibility to review this disclaimer regularly for any changes.